Loading
Get Medcom Forms
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Medcom Forms online
Filling out the Medcom Forms online is a straightforward process that allows users to submit claims efficiently. This guide provides step-by-step instructions to ensure accurate completion of the form and a seamless submission experience.
Follow the steps to complete the Medcom Forms online.
- Click ‘Get Form’ button to obtain the Medcom Forms and open it in your preferred editor.
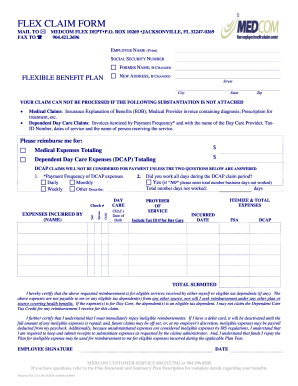
- Begin by entering your employee name and social security number in the designated fields. If your name has changed, provide your former name as well.
- Update your address if it has changed. Fill in your new street address, city, state, and zip code accurately.
- Attach the necessary substantiation documents. For medical claims, include an insurance explanation of benefits and a medical provider invoice. For dependent day care claims, provide itemized invoices, tax ID numbers, and details regarding the dates of service.
- Indicate the total amount for medical expenses and dependent day care expenses. Ensure the totals correspond to the attached documentation.
- If you are filing a dependent care assistance program (DCAP) claim, answer the provided questions regarding payment frequency and confirmation of workdays during the claim period.
- Itemize your expenses in the dedicated section, including the provider's name, date incurred, and the total submitted.
- Review the certification statement and ensure you agree to all stipulations outlined. This is necessary to proceed with your claim submission.
- Finally, sign and date the form to certify its accuracy and completeness. Saving your changes and documentation is essential before submitting your claim.
- You may save changes, download the completed form, print it for your records, or share it as necessary.
Start filling out your Medcom Forms online today for a streamlined claims experience!
Get form
Experience a faster way to fill out and sign forms on the web. Access the most extensive library of templates available.
Get This Form Now!
Use professional pre-built templates to fill in and sign documents online faster. Get access to thousands of forms.