Loading
Get 18002912634
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the 18002912634 online
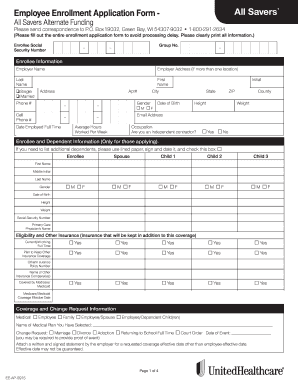
Filling out the 18002912634 form is an important step in your enrollment process. This guide provides clear instructions to help you complete the form efficiently, ensuring that all necessary information is accurately provided to avoid processing delays.
Follow the steps to fill out the form correctly.
- Click the ‘Get Form’ button to obtain the form and open it in the editor.
- Begin with the enrollee information section. Enter the enrollee's Social Security number and group number. Clearly print all details to ensure readability.
- Fill in the employer's name and address. If applicable, include multiple locations to avoid any confusion.
- Input the enrollee's last name, first name, marital status, address, phone numbers, date employed full time, gender, date of birth, height, weight, email address, average hours worked per week, occupation, and whether they are an independent contractor.
- If applying for dependents, provide information for each, including their names, relationship, gender, date of birth, height, weight, and Social Security number.
- In the eligibility and other insurance section, specify whether the enrollee or dependents have any other existing insurance coverage, and provide all necessary details of the other insurance policies.
- Complete the medical history section thoroughly, answering all questions regarding previous health conditions or treatments. Be honest and provide explanations where necessary.
- Fill out any prior medical coverage information if applicable, including details about previous plans or coverage.
- Review the signature section. Confirm that all statements are true and correct, and sign with the date. If signed by a representative, indicate their authority.
- If waiving medical coverage, complete the waiver section, stating the reason for waiving and any qualifying coverage details.
- Finally, ensure that all pages are attached and complete before finalizing. Users can save changes, download, print, or share the completed form as needed.
Start filling out your 18002912634 form online now!
Alternate Funding products are marketed under the All Savers brand. Excess Loss insurance coverage is provided by All Savers Insurance Company, a UnitedHealthcare company. The underlying medical coverage for the Alternate Funding products is not an insured product.