Loading
Get Health Care Provider Certification (hcpc) For Medical Leave
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Health Care Provider Certification (HCPC) For Medical Leave online
The Health Care Provider Certification (HCPC) For Medical Leave is an essential document used to request medical leave for yourself or an immediate family member. This guide provides detailed, step-by-step instructions to help you complete the form accurately online, ensuring a smooth submission process.
Follow the steps to complete the HCPC For Medical Leave form online.
- Click ‘Get Form’ button to obtain the form and open it in the editor.
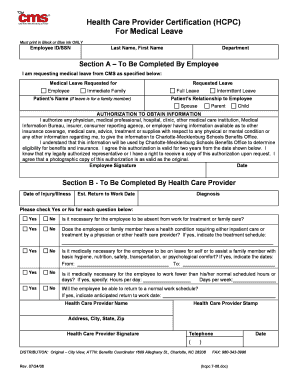
- In the first section labeled 'Employee ID/SSN', enter your employee identification number or Social Security Number as prompted.
- Fill in your last name and first name in the designated fields to identify yourself.
- Specify your department in the provided space, ensuring accurate alignment with your workplace records.
- In Section A, indicate whether you are requesting leave for yourself or an immediate family member by selecting 'Medical Leave Requested for Employee' or 'Immediate Family' as appropriate.
- If you are requesting leave for a family member, provide the patient’s name.
- Choose the type of leave you are requesting: 'Full Leave' or 'Intermittent Leave' by selecting the appropriate option.
- State the relationship of the patient to you by checking one of the following options: 'Spouse', 'Parent', or 'Child'.
- In the 'Authorization to Obtain Information' section, review the statement. Your signature and date are required, affirming your consent to share relevant medical information.
- Proceed to Section B, which must be completed by your health care provider. Ensure your provider fills in the 'Date of Injury/Illness' and 'Estimated Return to Work Date'.
- The health care provider should enter the diagnosis in the designated area.
- For each of the subsequent questions in this section, the health care provider should check 'Yes' or 'No' as relevant, providing additional details where necessary.
- If applicable, the health care provider should specify any treatment schedule and the duration of leave needed for you or your family member.
- The health care provider must provide their stamp, name, address, and signature, along with their telephone number.
- After ensuring all sections are accurately filled, review the form for completeness. You can then save changes, download a copy, print the form, or share it as needed.
Complete your Health Care Provider Certification (HCPC) For Medical Leave online today to ensure timely processing of your request.
“Serious health condition” means an illness, injury, impairment, or physical or mental condition that involves…” 8 sections to the definition of serious health condition in statute. Generally includes chronic serious health conditions, mental health conditions, substance abuse treatment, and others.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.