Loading
Get Patient Assistance Program Application
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Patient Assistance Program Application online
Completing the Patient Assistance Program Application online can be a straightforward process when you understand the necessary steps and information required. This guide will walk you through each section of the application to ensure that you fill it out accurately and completely.
Follow the steps to successfully complete your application online.
- Press the ‘Get Form’ button to retrieve the application form and open it in your online editor.
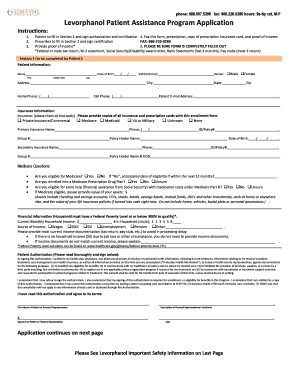
- Begin with Section 1, where the patient must provide their personal information including name, date of birth, gender, and contact details. This section must be signed for authorization and certification.
- Next, fill out the insurance information. Indicate if you have private insurance, Medicare, Medicaid, or none. Provide details about your primary and secondary insurances, including names, phone numbers, and policy numbers.
- Answer the Medicare questions to establish your eligibility. Include information on your assets if applicable.
- In the financial information section, report your current monthly household income and the number of individuals in your household. Provide documents to verify your income or indicate if your income is currently $0.
- Complete the patient authorization form, ensuring to read the terms before signing and dating the application.
- Fill out Section 2, designed for the prescriber. This includes the prescriber’s details such as name, license number, facility information, and medical information of the patient.
- The prescriber must certify and sign the application, affirming that the provided information is accurate and complete.
- After filling out all sections of the form, ensure that everything is complete. Save your changes, and then download, print, or share the application as needed.
Complete your Patient Assistance Program Application online today!
The Emergency Prescription Assistance Program, or EPAP, helps people in a federally-identified disaster area who do not have health insurance get the prescription drugs, vaccinations, medical supplies, and equipment that they need.