Loading
Get Mn Bcbs X20959 2018-2026
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the MN BCBS X20959 online
This guide provides clear and comprehensive instructions for completing the MN BCBS X20959 form online. Users can follow these steps to ensure accurate submission and adherence to the necessary guidelines.
Follow the steps to fill out the MN BCBS X20959 form effectively.
- Click the ‘Get Form’ button to obtain the necessary form and open it in your document editor.
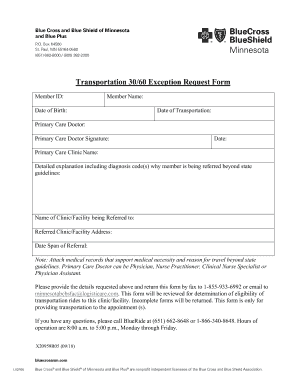
- Begin filling out the form by entering the Member ID, which is a unique identifier for each member.
- Next, populate the Member Name field with the full name of the member requesting transportation.
- Enter the Date of Birth for the member to provide additional identification.
- Fill in the Date of Transportation to indicate the desired date for travel.
- Provide the Primary Care Doctor's name, who is responsible for the referral.
- Sign the form in the space designated for the Primary Care Doctor Signature.
- Include the Date on which the signature was made.
- Enter the Primary Care Clinic Name to indicate where the primary care doctor practices.
- In the section that asks for a detailed explanation, thoroughly describe the diagnosis and the reasons for referring the member outside state guidelines, including any relevant diagnosis codes.
- Specify the Name of the Clinic/Facility being referred to for the appointment.
- Fill in the Referred Clinic/Facility Address to ensure accurate routing of the form.
- Indicate the Date Span of Referral to clarify the time frame for travel.
- Attach supporting medical records that justify the medical necessity for transportation beyond state guidelines.
- After completing all fields, review the form to ensure all entries are accurate and complete.
- Save the changes made to the form, then download or print it as needed.
- Finally, share the completed form by faxing it to 1-855-933-6992 or emailing it to minnesotabcbsfac@logisticare.com.
Complete your MN BCBS X20959 form online today to ensure timely processing.
Call (651) 662-5050, 1-800-262-0823. Email.