Loading
Get Activity Prescription Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Activity Prescription Form online
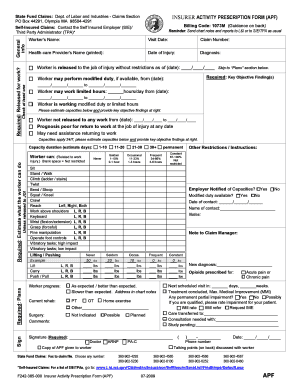
The Activity Prescription Form is a crucial document used to communicate a worker's capacity and restrictions after an injury. This guide will provide you with step-by-step instructions on how to fill out the form online, ensuring clear and accurate information submission.
Follow the steps to complete the Activity Prescription Form online effectively.
- Press the ‘Get Form’ button to obtain the Activity Prescription Form and open it in your browser or preferred editor.
- Enter the worker’s name in the designated field. Ensure that the name matches the identification used in official records.
- Input the visit date to reflect the date when the assessment was made. Use the MM/DD/YYYY format to maintain consistency.
- Fill in the claim number associated with the worker's insurance case. This helps in tracking the claim efficiently.
- Print the name of the health-care provider completing the form in the provided field.
- Record the date of injury. This should also follow the MM/DD/YYYY format as previously noted.
- Indicate the diagnosis clearly, ensuring that it is accurate and relevant to the injury.
- Specify if the worker is released to the job of injury without restrictions as of a particular date. If applicable, record the date in the designated field.
- Provide any key objective finding(s) that support the recommended activity levels for the worker.
- Indicate whether the worker is able to perform modified duty and fill in the range of dates during which this applies.
- If applicable, specify any limited hours the worker may be able to work per day and the period these hours apply.
- Estimate the worker’s capacities in the provided section, noting any restrictions or instructions that need to be followed.
- Fill out the employer notification section to confirm if the employer has been informed of the worker's capacities.
- Review all sections to confirm that the information is complete and accurate before saving changes.
- Once completed, you can save your changes, download the form for your records, or print it out for submission.
Complete your Activity Prescription Form online today for a streamlined process.
Employees may also file a claim form online at http://.lni.wa.gov/ORLI/ECS/FileFast.asp or by phone at 1-877-561-FILE (3453). Workers' compensation claims must be filed within one year of an injury, and within two years of being notified that an illness is work-related.