Loading
Get Emi Health Cobra Continuation Application
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the EMI Health COBRA Continuation Application online
Completing the EMI Health COBRA Continuation Application is an essential step for anyone looking to continue their health insurance coverage following a qualifying event. This guide will provide you with clear and concise instructions to help you fill out the application online with confidence.
Follow the steps to complete your application accurately.
- Press the 'Get Form' button to access the EMI Health COBRA Continuation Application form. This will enable you to open the document and begin the completion process.
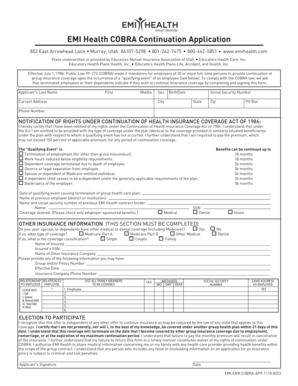
- Start by filling in the applicant's name, including last name, first name, and middle name. Ensure that all fields are completed accurately for identification purposes.
- Provide the applicant's sex and birth date, making sure to format the date correctly. Input the Social Security Number (SSN) as it is required for processing your application.
- Enter the current address, including city, state, zip code, and PO Box if applicable. Accurate address information is vital for communication regarding your coverage.
- Input the phone number where you can be reached. This should be a valid phone number to facilitate any necessary follow-up.
- Read the notification of rights under the Continuation of Health Insurance Coverage Act of 1986 carefully, ensuring you understand your entitlements and obligations.
- Select the qualifying event that applies by marking the appropriate checkbox. Examples include termination of employment, reduced work hours, and other listed events.
- Document the date of the qualifying event and the name of the previous employer, along with the name and Social Security Number of the previous EMI Health contract holder.
- Indicate the desired coverage by checking only the employer-sponsored benefits you wish to continue, such as medical, dental, or vision.
- Complete the SECTION ON OTHER INSURANCE INFORMATION, indicating whether you or any dependents have other medical or dental coverage. Provide details regarding other insurance if applicable.
- List all family members to be covered by the continuation of coverage, including their sex, birthdate, Social Security number, and whether they share the same address as the employee.
- Review the election to participate statement carefully. Read understanding your coverage limitations and certify by providing your signature and the date at the end of the form.
- After filling out all sections of the form, make sure to save your changes, and then proceed to download, print, or share the completed application as needed.
Take the next step in securing your health coverage by completing the EMI Health COBRA Continuation Application online today.
If you elect for COBRA, then cancel it, you are not eligible to elect COBRA again on that health plan. You can use COBRA benefits again should you get another job and have health insurance through them and then were laid off.