Get Aetna Coordination Of Benefits Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Aetna Coordination Of Benefits Form online
Filling out the Aetna Coordination Of Benefits Form is an important step in ensuring that your medical claims are processed accurately. This guide will provide you with the necessary steps to complete the form effectively online, ensuring that all relevant information is captured to optimize coverage.
Follow the steps to accurately complete the Aetna Coordination Of Benefits Form
- Click ‘Get Form’ button to obtain the form and open it in the editor.
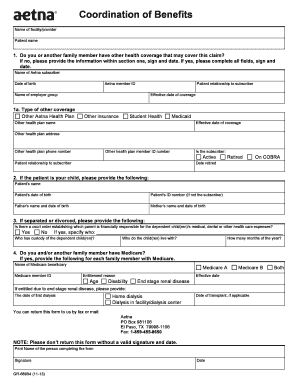
- Begin by entering the name of the facility or provider along with the patient's name in the designated fields.
- Answer the first question regarding other health coverage. If you or a family member does have other health coverage that may cover the claim, make sure to fill out all fields. If not, you can simply provide the information in section one, then sign and date the form.
- Provide the name of the Aetna subscriber along with their date of birth and Aetna member ID.
- Indicate the patient's relationship to the subscriber and the name of the employer group.
- In section 1a, specify the type of other coverage, including options like ‘Other Aetna Health Plan,’ ‘Medicaid,’ or ‘Student Health’.
- Fill in the effective date of coverage for the other insurance and provide the name, address, and phone number of the other health plan.
- Include the other health plan member ID number and clarify the patient's relationship to the subscriber in this section.
- Determine if the subscriber is active, retired, or on COBRA, and provide relevant dates if applicable.
- If the patient is a child, provide the patient’s details including their name, date of birth, and ID number, along with the names and dates of birth of both parents.
- If applicable, complete the section regarding custody and financial responsibility, indicating if there is a court order and specifying who has custody of the dependent children.
- Answer the question regarding Medicare coverage and include necessary details for each family member who has Medicare, including their beneficiary name and member ID.
- If applicable, fill in the date of first dialysis and any other necessary information regarding medical history.
- Finally, ensure that the form is signed and dated by the person completing it, providing their printed name.
- Save your changes, and then download, print, or share the form as needed.
Complete your Aetna Coordination Of Benefits Form online today to ensure your claims are processed without delay.
Coordination of benefits (COB) allows plans that provide health and/or prescription coverage for a person with Medicare to determine their respective payment responsibilities (i.e., determine which insurance plan has the primary payment responsibility and the extent to which the other plans will contribute when an ...
Fill Aetna Coordination Of Benefits Form
NOTE: Please don't return this form without a valid signature and date. Print Name of the person completing the form. Signature. Date. Coordination of benefits (COB) is a process that identifies which health plan is primary when a patient has more than one plan. We created this guide to help providers submit their COB claims electronically. Enrollee Signature. Date. Coordination of Benefits Request Form. Please answer all of the questions below and return this form to the Chevron Phillips Employee. Confirm that your practice management system and your vendor can create or forward coordination of benefits (COB) claims in the full Health Insurance. Coordination of Benefits (COB) Form.
Industry-leading security and compliance
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.