Loading
Get Nv Form C-3 2020-2026
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the NV Form C-3 online
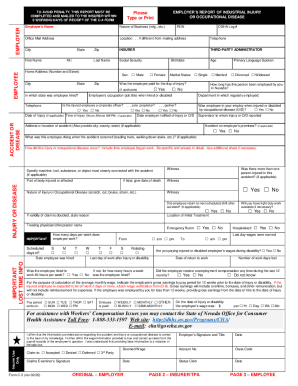
Filling out the NV Form C-3 online is an essential part of reporting industrial injuries or occupational diseases. This guide provides clear, step-by-step instructions to ensure you complete the form accurately and efficiently.
Follow the steps to complete the NV Form C-3 online.
- Press the ‘Get Form’ button to acquire the form and open it in your browser for editing.
- Begin by entering the employer’s name and nature of business in the relevant fields. Make sure these details are accurate.
- Fill in the office mailing address along with the location if it's different from the mailing address. Provide a contact telephone number and zip code.
- Next, complete the insurer and third-party administrator sections, including last name, first name, social security number, and address details.
- For the employee section, fill in the employee's full name, home address, age, and marital status. Specify the employee's sex by selecting Male or Female.
- Indicate whether the employee was paid for the day of the injury and their status as a sole proprietor or partner.
- Record the date and time of the injury, and the date the employer was notified. Ensure all information provided is as precise as possible.
- Detail the location of the accident, the action the employee was performing at the time, and how the injury occurred. Use as much space as necessary for clarity.
- If applicable, provide information about witnesses to the accident and any machines or tools involved.
- Complete the injury or disease section with specific details about the nature of the injury and any follow-up actions required.
- Confirm if the injured employee returned to their next scheduled shift, if light duty work is available, and if the employee was hospitalized.
- In the lost time information section, fill in the employee’s work schedule, hire date, and their hours/week for the job.
- Finally, review all sections for accuracy. Save your changes, and choose whether to download, print, or share the completed form.
Complete your NV Form C-3 online to streamline the process of reporting industrial injuries and occupational diseases.