Get Ca E3065 2015
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the CA e3065 online
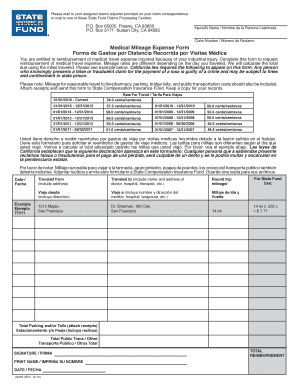
The CA e3065 form is a medical mileage expense form that allows individuals to request reimbursement for travel expenses related to medical appointments due to an industrial injury. This guide will help you navigate through the form step-by-step, ensuring that you complete it accurately and effectively.
Follow the steps to correctly complete the CA e3065 form.
- Click the ‘Get Form’ button to obtain the CA e3065 form and open it in your preferred electronic document editor.
- Enter the injured person's name in the designated field as it appears on your claims correspondence.
- Fill in the claim number provided in your claim correspondence. This information is essential for processing your reimbursement request.
- Document the travel dates by indicating each relevant date when travel to medical appointments occurred.
- For each trip, specify the starting address and the destination address related to your medical appointments, including the name and address of the provider.
- Calculate the round trip mileage for each journey and enter that information in the mileage box.
- Refer to the mileage rate table to determine the applicable rate for the dates of your travels. Input this information to calculate your total reimbursement.
- Include any additional travel-related expenses such as parking fees or tolls. Remember to attach receipts for these expenses.
- Sign and date the form to authenticate your request for reimbursement.
- After thoroughly reviewing the completed form for accuracy, save your changes, then download, print, or share the form as needed.
Complete your CA e3065 form online today for a seamless reimbursement experience!
Get form
To obtain a California Community College teaching credential, you must meet specific educational and professional requirements outlined by the California Community Colleges Chancellor's Office. Completing necessary applications and submitting your transcripts are essential steps. For any official forms you may need, including the CA e3065, platforms like uslegalforms can be an invaluable resource.