Get Ny Doh-4156 2014-2026
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the NY DOH-4156 online
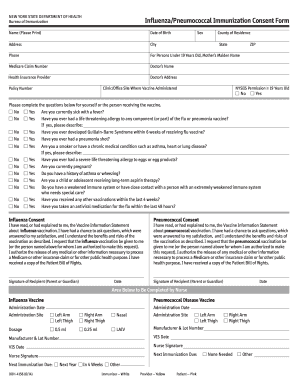
This guide provides a comprehensive overview of how to fill out the NY DOH-4156, the Influenza/Pneumococcal Immunization Consent Form, online. Following these instructions will help ensure that all necessary information is accurately captured for vaccination purposes.
Follow the steps to complete the NY DOH-4156 form online.
- Click ‘Get Form’ button to obtain the form and open it in your chosen editor.
- Begin by entering your name in the designated field. Ensure that you print your name clearly.
- Input your date of birth in the specified format, typically MM/DD/YYYY.
- Indicate your sex by selecting the appropriate option from the dropdown menu.
- Fill in your county of residence as well as your complete address, including city, state, and ZIP code.
- Provide your phone number for contact purposes in case additional information is needed.
- If you are filling out this form for a person under 19 years old, include the mother’s maiden name as requested.
- Enter the Medicare claim number if applicable, as well as the name of the attending doctor and their contact address.
- Indicate the name of your health insurance provider along with the policy number.
- Answer the medical screening questions by selecting 'Yes' or 'No' for each condition listed.
- Review the consent sections for both the influenza and pneumococcal vaccinations, then confirm your understanding by signing and dating in the allocated areas.
- Ensure that the form is completed in full and review all entries for accuracy.
- Finally, save any changes made to the document. You can then download it, print the completed form for your records, or share it as needed.
Complete your immunization documents online today for a hassle-free experience.
You may not be eligible for the flu vaccine due to certain medical conditions that compromise your immune system, or if you have a history of severe allergic reactions to vaccine components. Additionally, specific age restrictions could apply. It's crucial to review the NY DOH-4156 criteria to confirm your eligibility. Discussing your health concerns with a healthcare provider can clarify your options.