Loading
Get Ny Health Care Flexible Spending Account (hcfsa) Program Claims Form 2019
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the NY Health Care Flexible Spending Account (HCFSA) Program Claims Form online
Filling out the NY Health Care Flexible Spending Account (HCFSA) Program Claims Form online can streamline your reimbursement process for eligible health care expenses. This guide will provide you with expert instructions on how to accurately complete each section of the form.
Follow the steps to complete the claims form easily and accurately.
- Click ‘Get Form’ button to obtain the form and open it for completion.
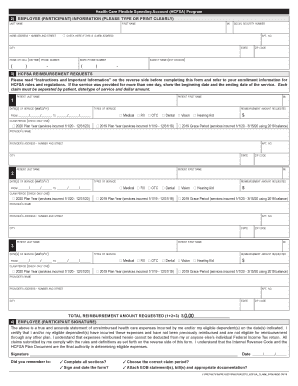
- In the 'Employee (Participant) Information' section, type or print clearly your last name, middle initial, first name, home address, social security number, phone numbers, and agency name. If you have moved recently, check the box indicating a new address.
- Navigate to the 'HCFSA Reimbursement Requests' section. Here, list the patient’s name, dates of service, type of service, provider’s information, and the reimbursement amount requested. Make sure to provide separate details for each claim involving different patients or services.
- In the claim period section, select the appropriate option indicating the service dates by checking the relevant box. Consider if the expenses were incurred during the current plan year, the previous plan year, or the grace period for claims.
- After entering all claims, calculate the total reimbursement amount requested by adding individual amounts in the designated area.
- Proceed to the 'Employee (Participant) Signature' section. Sign and date the form, certifying the accuracy of the information provided and confirming that these expenses have not been reimbursed via another plan.
- Before submitting, review the form to ensure that all sections are completed, the form is signed and dated, and the correct claim period is selected. Gather and attach all necessary documentation, such as itemized bills and EOB statements.
- Finally, save your changes, download, print, or share the completed claims form as required before submitting it to the designated address.
Complete your reimbursement request online today for a smoother financial experience.
Get form
Experience a faster way to fill out and sign forms on the web. Access the most extensive library of templates available.
Related links form
Get This Form Now!
Use professional pre-built templates to fill in and sign documents online faster. Get access to thousands of forms.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.