Get Wellcare Medicare Coverage Determination Request Form 2007-2026
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the WellCare Medicare Coverage Determination Request Form online
Filling out the WellCare Medicare Coverage Determination Request Form is an essential step in obtaining necessary coverage for medications. This guide provides detailed instructions to help you successfully complete and submit the form online.
Follow the steps to fill out the WellCare Medicare Coverage Determination Request Form with ease.
- Press the ‘Get Form’ button to access the WellCare Medicare Coverage Determination Request Form and open it in your preferred editor.
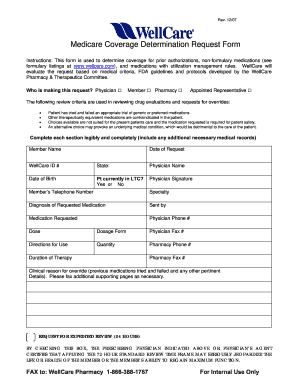
- Identify who is making the request by selecting the appropriate option: Physician, Member, Pharmacy, or Appointed Representative.
- Fill in the 'Member Name' field with the full name of the person requesting the medication coverage.
- Enter the 'Date of Request' in the specified format to indicate when the request is being made.
- Input the 'WellCare ID #' assigned to the member for proper identification.
- Complete the 'State' field, indicating the state of the member’s residence.
- Provide the 'Physician Name' who is making the request.
- Include the 'Date of Birth' of the member to confirm their identity.
- Indicate if the patient is currently in long-term care by selecting 'Yes' or 'No'.
- Ask the physician to provide their 'Signature' to validate the request.
- Fill out the 'Member’s Telephone Number' for any necessary follow-up.
- Specify the 'Specialty' of the physician to identify their area of expertise.
- Detail the 'Diagnosis of Requested Medication' to justify the request.
- Enter the 'Medication Requested' that is being sought.
- List the 'Physician Phone #' for further communication regarding the request.
- Specify the 'Dose' required for the medication.
- Select the 'Dosage Form' that corresponds to the requested medication.
- Provide the 'Physician Fax #' for document submission.
- Write the 'Directions for Use' for the medication to ensure proper administration.
- Indicate the 'Quantity' of the medication needed.
- Include the 'Pharmacy Phone #' for direct contact for any prescription queries.
- Mention the 'Duration of Therapy' for which the medication is requested.
- Provide the 'Pharmacy Fax #' for sending additional documents if required.
- Explain the 'Clinical reason for override,' detailing previous medications tried and pertinent information.
- If expedited review is needed, check the box indicating that applying the standard review time may jeopardize the member’s health.
- After completing all fields, save changes, download, print, or share the form as necessary.
Now that you have the steps, complete the WellCare Medicare Coverage Determination Request Form online to ensure timely access to your necessary medications.
A coverage determination is a decision made by WellCare regarding whether a specific service or medication is covered under your plan. This process often involves the use of the WellCare Medicare Coverage Determination Request Form to include all necessary details about the requested service. Understanding this concept can help you verify if you need prior authorization.