Loading
Get Of Form Cob Questionnaire
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Of Form Cob Questionnaire online
Filling out the Of Form Cob Questionnaire accurately is essential for managing health coverage and ensuring proper coordination of benefits. This guide provides a comprehensive approach to completing the form online, aiming to assist users in navigating its components effectively.
Follow the steps to fill out the Of Form Cob Questionnaire online with ease.
- Click ‘Get Form’ button to obtain the form and open it in the editor.
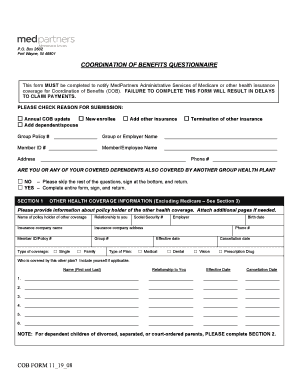
- Review the reason for submission section at the top of the form. Choose one of the available options, including annual COB update, new enrollee, add other insurance, termination of other insurance, or add dependent/spouse. Mark the appropriate box to indicate your submission reason.
- Fill in the group policy number and the group or employer name. Make sure to provide accurate information to avoid delays.
- Enter your member ID number and your name in the designated fields. Ensure that the name is spelled correctly as it appears in your documentation.
- Complete your address and phone number. Make sure to provide current contact details so that you can be reached if needed.
- Indicate whether you or any covered dependents are also covered by another group health plan. If the answer is ‘No’, please skip to the signature section at the end. If ‘Yes’, proceed to fill in the subsequent sections.
- In Section 1, provide information about the policyholder of the other health coverage. Include details such as their name, relationship to you, Social Security number, employer, birth date, insurance company name and address, phone number, member ID/policy number, group number, effective date, cancellation date, and type of coverage (single or family).
- List who is covered by this other plan. Include your name if applicable and provide the effective and cancellation dates for each covered person.
- If applicable, complete Section 2 regarding special situations for dependent children. Indicate if there is a court order for healthcare coverage and attach a copy if necessary. Provide details about the person responsible for the child’s health coverage.
- In Section 3, answer questions regarding Medicare coverage for you or your spouse. Indicate if you are covered by Medicare and provide necessary details regarding the effective dates for Hospital Part A and B.
- Sign and date the form in the designated area at the bottom of the document. This step is crucial as it confirms the accuracy of the information provided.
- Once you have completed the form, save your changes, download a copy if needed, print it out, or share it according to the submission instructions provided.
Ready to complete your Of Form Cob Questionnaire online? Start now to ensure your health benefits are coordinated effectively.
Coordination of benefits (COB) allows plans that provide health and/or prescription coverage for a person with Medicare to determine their respective payment responsibilities (i.e., determine which insurance plan has the primary payment responsibility and the extent to which the other plans will contribute when an ...
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.