Loading
Get Wi F-44192 2017
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the WI F-44192 online
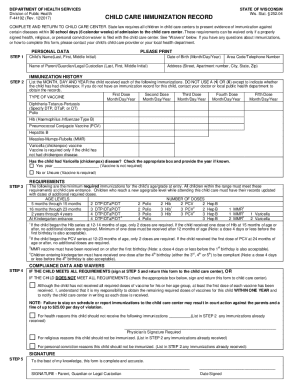
The WI F-44192 is an essential form for documenting immunization records required for children attending child care centers in Wisconsin. This guide will provide clear instructions on completing the form accurately and efficiently online.
Follow the steps to complete the WI F-44192 form online.
- Click ‘Get Form’ button to obtain the form and open it in the editor.
- Begin by filling in the personal data of the child. Please print the child’s name clearly, including last name, first name, and middle initial. Next, enter the date of birth using the month/day/year format. Include the appropriate area code and telephone number, followed by the name of the parent, guardian, or legal custodian in the same format. Finally, provide the complete address, including street, apartment number (if applicable), city, state, and zip code.
- For immunization history, list the month, day, and year the child received each required immunization. Do not use a check mark or X, except to indicate whether the child has had chickenpox. Ensure that all vaccinations are accurately recorded under the respective vaccine type, along with their corresponding dates.
- In the requirements section, review the minimum immunization requirements according to the child's age and grade at entry. Ensure that the child has received the stipulated number of doses for each vaccine. This ensures compliance; if the child has not received all necessary doses, select the appropriate checkbox and acknowledge the responsibility for obtaining the remaining doses within one year.
- The final step is to sign the form. This signature confirms that to the best of your knowledge, the information provided is complete and accurate. Include the date signed, ensuring that all required fields have been filled out before submission.
Complete your forms online today to ensure your child's compliance with immunization requirements.
Get form
Experience a faster way to fill out and sign forms on the web. Access the most extensive library of templates available.
Get This Form Now!
Use professional pre-built templates to fill in and sign documents online faster. Get access to thousands of forms.