Loading
Get C1 Form Workers Comp
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the C1 Form Workers Comp online
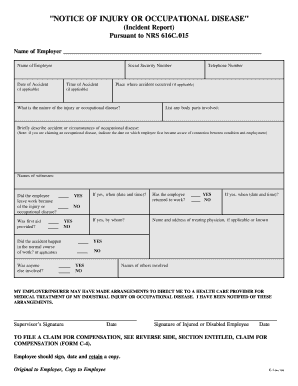
Filling out the C1 Form for Workers Compensation is an important step in reporting an injury or occupational disease. This guide provides a clear and comprehensive walkthrough of each section to ensure that you can complete the form accurately and effectively online.
Follow the steps to complete the C1 Form Workers Comp online.
- Press the ‘Get Form’ button to retrieve the form and display it in the editor.
- Begin by entering the name of your employer in the designated field. This information is essential for identifying the entity responsible for workers' compensation.
- Next, provide your name as the employee. Ensure that it matches your identification documents.
- Fill in your Social Security Number in the specified field. This is necessary for tracking and processing your claim.
- Document the date of the accident in the appropriate section. If the incident relates to an occupational disease, include the date you first recognized the connection with your employment.
- Indicate the time of the accident, if applicable, to provide a complete account of the incident.
- Input your telephone number so that the employer or claims personnel can contact you if further information is needed.
- Describe the place where the accident took place, marking it as applicable.
- Specify the nature of the injury or occupational disease you experienced. Be as detailed as necessary for clarity.
- List any body parts that were involved in the incident, ensuring to detail all injuries sustained.
- Provide a brief description of the accident or the circumstances surrounding the occupational disease. If claiming an occupational disease, clearly indicate the date of awareness regarding the connection to employment.
- Names of witnesses should be recorded, as they can provide supporting accounts if needed.
- Indicate whether you left work because of the injury or occupational disease, answering YES or NO.
- If treatment was received, specify when first aid was provided, including the date and time.
- Answer whether you have returned to work after the injury or disease, detailing by whom, if applicable.
- Provide the name and address of your treating physician, if known.
- Confirm whether the accident occurred during the normal course of work, and indicate if any other individuals were involved.
- Sign and date the form to certify the information provided is accurate. Ensure to obtain your supervisor's signature as well.
- After completing all fields, save the changes and choose to download, print, or share the form as necessary.
Complete your C1 Form Workers Comp online today for a smoother claims process.
C4 forms are required when billing for medical services related to workers' compensation when a patient was injured on the job. Workers compensation insurance will pay for all sorts of medical benefits. The board needs a copy of every workers comp claim filed. ...