Loading
Get Cms-1763 2017-2026
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the CMS-1763 online
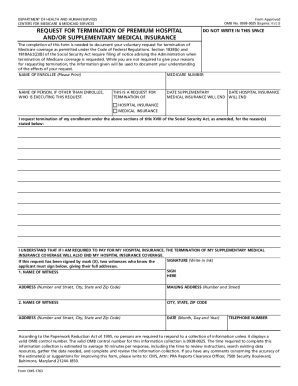
Filling out the CMS-1763 form is an essential process for individuals wishing to voluntarily terminate their Medicare coverage. This guide provides step-by-step instructions to help you complete the form accurately and efficiently.
Follow the steps to complete the CMS-1763 form
- Press the ‘Get Form’ button to access the CMS-1763 form and open it in the online editor.
- In the 'Name of enrollee' section, clearly print your full name. This ensures accurate identification and processing of your request.
- Enter your Medicare number in the designated field. This number is essential for verifying your enrollment status.
- If the request is being executed by a person other than the enrollee, fill out their name in the section labeled 'Name of person, if other than enrollee, who is executing this request.'
- Indicate the type of insurance coverage you are requesting to terminate by checking the appropriate boxes for supplementary medical insurance and/or hospital insurance.
- Specify the date you wish for the supplementary medical insurance and hospital insurance to end in the respective fields.
- In the reasons section, provide any necessary information regarding why you are requesting termination of your Medicare coverage. While this is not obligatory, it may be helpful.
- Sign the form in ink to validate your request. Ensure your signature is clear and legible to avoid processing delays.
- If the request is signed by mark (X), two witnesses must provide their signatures and full addresses in the designated witness sections.
- Complete the mailing address, date, and telephone number sections to ensure your request can be processed accurately.
- Once all fields are completed, you can save your changes, download the document for your records, print it out, or share it as needed.
Take action now to complete your CMS-1763 form online and manage your Medicare coverage effectively.
In most cases, if you don't sign up for Medicare Part B when you're first eligible, you'll have to pay a late enrollment penalty. You'll have to pay this penalty for as long as you have Part B and could have a gap in your health coverage.