Loading
Get Prescription Drug Prior Authorization Request Form - Ccah-alliance
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Prescription Drug Prior Authorization Request Form - Ccah-alliance online
Completing the Prescription Drug Prior Authorization Request Form - Ccah-alliance online is a straightforward process designed to ensure that all relevant information is accurately captured for review. This guide will provide you with step-by-step instructions to fill out the form effectively.
Follow the steps to complete the form successfully.
- Press the ‘Get Form’ button to access the Prescription Drug Prior Authorization Request Form and open it in your preferred editor.
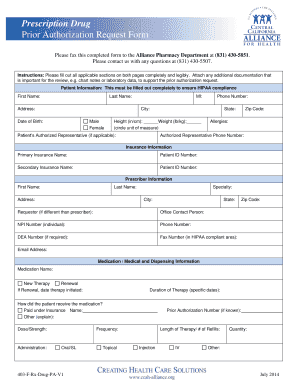
- Begin by filling out the patient information section completely. This includes the patient's first name, last name, address, phone number, date of birth, sex, height, weight, and any allergies. This information is crucial for HIPAA compliance.
- Next, provide the insurance information. Fill out the primary and secondary insurance names along with the corresponding patient ID numbers.
- Complete the prescriber information section. Include the prescriber's first name, last name, address, specialty, contact details, NPI number, DEA number (if applicable), and email address.
- In the medication/medical and dispensing information section, specify the medication name, whether it's a new therapy or a renewal, and provide details such as therapy duration, dosage, frequency, and administration method.
- Detail the patient's previous medication history concerning the current condition, including previous therapies, their durations, reasons for failure, and any allergies related to those medications.
- List the relevant diagnoses using ICD-9 or ICD-10 codes as appropriate.
- Gather and input any required clinical information, such as symptoms, laboratory results with dates, and justification for therapy. Ensure that this section is thoroughly filled out to support the prior authorization request.
- Review the entire form for accuracy and ensure all required sections are filled out. Provide any necessary attachments to support the request.
- Finally, complete the attestation at the end of the form, including the prescriber’s signature and date. Save your changes, and you may then download, print, or share the completed form as needed.
Begin your form completion process online today to ensure a timely review of your prior authorization request.
The GHPP is a prior authorization program. This means that a Service Authorization Request (SAR) must be submitted to the GHPP State office for approval for all diagnostic and treatments services, except for emergencies.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.