Loading
Get Owcp 5c
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Owcp 5c online
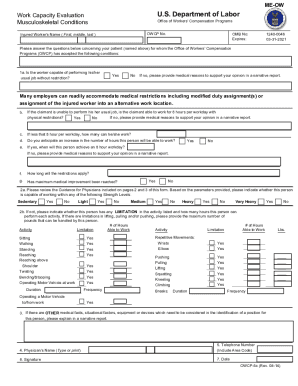
The Owcp 5c form is essential for providing detailed information about an injured worker's capacity to perform their job. This guide offers clear instructions on how to fill out the form online, ensuring that you understand each section and can complete it accurately.
Follow the steps to fill out the Owcp 5c form online.
- Press the ‘Get Form’ button to acquire the form and open it in the online editor.
- Enter the injured worker's name in the designated field, ensuring to include their first, middle, and last name.
- Address the question regarding whether the worker can perform their usual job without restrictions; select 'Yes' or 'No' accordingly.
- If 'No', provide detailed medical reasons in the narrative report section to support your opinion.
- Consult the subsequent questions about the worker's ability to work for 8 hours per workday, and respond with 'Yes' or 'No' based on their condition.
- If applicable, specify the number of hours the worker can work if it is less than 8 hours.
- Indicate whether you anticipate an increase in the hours the person can work in the future and provide a date, if applicable.
- Respond to questions about the medical improvements and any physical restrictions that apply, following the guidelines for sedentary to very heavy work levels.
- Complete the sections regarding the specific activities listed (e.g., sitting, standing, walking) and mark any relevant limitations.
- Fill in the physician's name, contact number, signature, and the date at the end of the form.
- Review your inputs to ensure all sections are complete, then save your changes, and choose to download, print, or share the completed form.
Take action now and complete the Owcp 5c form online to assist in the processing of claims.
CA-5. Subject. Claim for Compensation by Widow, Widower, and/or Children.