Loading
Get Solicitud De Informacin Sobre El Empleo. Formulario Cms L564/r297
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the SOLICITUD DE INFORMACION SOBRE EL EMPLEO. Formulario CMS L564/R297 online
This guide provides a clear and comprehensive approach to filling out the SOLICITUD DE INFORMACION SOBRE EL EMPLEO. Formulario CMS L564/R297 form online. Whether you are applying for Medicare or assisting someone else, the following steps will help you navigate through the process smoothly.
Follow the steps to effectively complete the form.
- Click ‘Get Form’ button to obtain the form and open it for online completion.
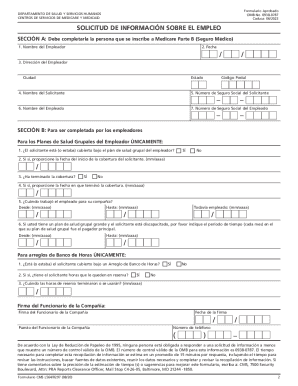
- In Section A, enter the following details: 1. Employer's name: Write the name of your employer. 2. Date: Fill in the date on which you are completing the form. 3. Employer's address: Provide the complete address of your employer, including city and state. 4. Applicant's name: Enter your full name. 5. Applicant's Social Security Number: Enter your Social Security number. 6. Employee's name: If you receive coverage based on your employment, fill in your name; otherwise, use the name of the person providing coverage. 7. Employee's Social Security Number: If applicable, provide the Social Security number of the person whose coverage you are using.
- Once Section A is complete, provide the form to your employer for them to fill out Section B.
- In Section B, the employer will provide information about the group health plan coverage: 1. Confirm if the applicant is (or was) covered under the employer's group health plan. 2. If covered, provide the start date of the applicant’s coverage in the format mm/yyyy. 3. Indicate whether the coverage has ended. 4. If applicable, provide the end date of coverage in the format mm/yyyy. 5. Document the employment dates for the relevant employee and indicate if they are still employed.
- If the applicant is a person with a disability, the employer must detail the period during which the group health plan was the primary payer.
- Complete any additional required information for hourly bank arrangements if applicable.
- Ensure that the employer's authorized representative signs and dates the form, completing their title and contact number for any follow-up inquiries.
- After both sections are filled out, review the information for accuracy, save the changes, and prepare to submit the completed form to the local Social Security office.
Start your application process today by completing the form online.
CMS Form Number. CMS-R-297. 2023-03-06. Request for Employment Information. CMS-R-297 cms.gov https://.cms.gov › legislation › pra-listing › cms-r-297 cms.gov https://.cms.gov › legislation › pra-listing › cms-r-297
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.