Loading
Get Acariahealth Oncology Urology Referral Form 2019-2025
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the AcariaHealth Oncology Urology Referral Form online
Filling out the AcariaHealth Oncology Urology Referral Form online is a crucial step in ensuring patients receive the necessary treatment efficiently. This guide provides clear, step-by-step instructions to help users accurately complete the form with confidence.
Follow the steps to accurately complete the form.
- Click ‘Get Form’ button to access the Oncology Urology Referral Form and open it in the online editor.
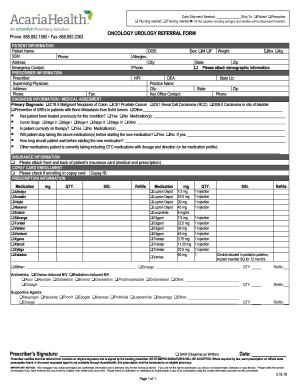
- Begin with the patient information section. Enter the patient's name, date of birth, sex, weight (in pounds or kilograms), social security number, phone number, allergies, and address details including city, state, and zip code. Don't forget to include an emergency contact's name and phone number. If available, attach demographic information.
- Proceed to the prescriber information section. Fill in the prescriber's name, NPI, DEA, state license, supervising physician details, practice name, and the complete address. Additionally, provide the prescriber’s phone and fax number, along with the key office contact's phone number.
- Complete the diagnosis information section. Specify the primary diagnosis by checking the appropriate box and, if necessary, detail if the patient has been treated for this condition before. Record any medications the patient has previously taken and indicate the cancer stage.
- Inquire if the patient is currently undergoing therapy. If so, list the medications they are on and whether they will discontinue them prior to starting a new medication. Offer details on the waiting period for initiating the new treatment.
- Collect insurance information. Remember to attach the front and back of the patient's insurance card, which includes both medical and prescription coverage.
- If applicable, check the box for copay card enrollment and provide the copay ID.
- Fill in the prescription information by selecting the relevant medications and providing dosages, quantity, instructions, and refill details.
- Include information for any required antimetics or supportive agents, detailing the dosage, quantity, and refills as applicable.
- Finally, the prescriber must sign the form to certify that the details are correct and complete. No stamped signatures will be accepted.
- Once all fields have been accurately filled, save the form, and opt to download, print, or share it as needed.
Ensure you complete essential documents online to facilitate proper patient care.
Envolve, through its family of companies, is a national specialty pharmacy provider offering comprehensive specialty drug management services focused on improving care and outcomes for patients living with complex conditions.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.