Loading
Get Authorization Of Disclosure/permission To Share Protected Health Information
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Authorization Of Disclosure/Permission To Share Protected Health Information online
Filling out the Authorization Of Disclosure/Permission To Share Protected Health Information form is a crucial step in managing your medical records. This guide will walk you through each section of the form, ensuring that you can complete it accurately and efficiently to authorize the sharing of your protected health information.
Follow the steps to complete the form successfully.
- Click ‘Get Form’ button to obtain the form and open it for editing.
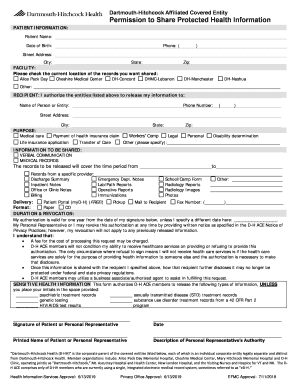
- Complete the patient information section by entering your name, date of birth, phone number, and mailing address including city, state, and zip code.
- In the facility section, indicate the location of the records you want shared by checking the appropriate box. This could be one of the Dartmouth-Hitchcock hospitals or another specified location.
- Fill in the recipient section by providing the name of the person or entity who will receive the information, their phone number, and mailing address.
- Select the purpose for sharing your health information by checking the box that best describes your reason. If none apply, check 'Other' and specify your purpose.
- In the information to be shared section, indicate whether you’re authorizing verbal communication, medical records, or both. Specify the time period of the records to be accessed.
- Choose the form of delivery for the records, such as patient portal, mail, or fax. Ensure you provide the preferred delivery method by checking the appropriate boxes.
- Select the format in which you'd like to receive the records, either in paper format or on an encrypted CD.
- In the duration and revocation section, note that your authorization is valid for one year unless otherwise stated. You may revoke this authorization anytime following the specified instructions.
- Review the sensitive health information section. If you do not want to release any specified sensitive information, place your initials in the space provided.
- Finally, sign and date the form. If you are not the patient, include a description of your relationship to the patient and any legal authority to sign.
- Save your changes, then download, print, or share the completed form as required.
Complete your document online to ensure a smooth process for sharing your protected health information.
An authorization is a detailed document that gives covered entities permission to use protected health information for specified purposes, which are generally other than treatment, payment, or health care operations, or to disclose protected health information to a third party specified by the individual.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.