Loading
Get Fax: 1-855-668-8552
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Fax: 1-855-668-8552 online
This guide provides a detailed overview of how to fill out the Fax: 1-855-668-8552 form for coverage determination requests. Follow these steps to ensure you complete the form accurately and effectively.
Follow the steps to successfully complete the coverage determination request form.
- Press the ‘Get Form’ button to acquire the form and open it in your desired editing program.
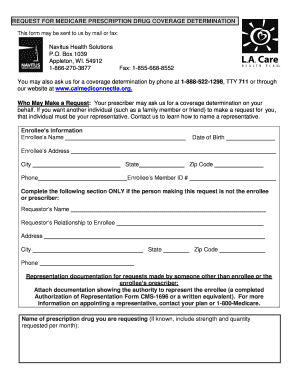
- Begin filling out the enrollee’s information, including their name, date of birth, address, city, state, zip code, and phone number. Ensure all details are accurate.
- Input the enrollee's member ID number accurately to facilitate processing.
- If the request is being made by someone other than the enrollee or prescriber, complete the requestor’s information section. Provide the requestor's name, relationship to the enrollee, address, city, state, zip code, and phone number.
- Attach any representation documentation showing the authority of the requestor to act on behalf of the enrollee, such as a completed Authorization of Representation Form or its equivalent.
- Specify the name of the prescription drug you are requesting, including the strength and quantity requested per month if known.
- Select the type of coverage determination request from the options provided. You may need to check additional specifics related to your request.
- If requesting an expedited decision, check the appropriate box and attach any supporting statement from the prescriber.
- Sign and date the form at the bottom where indicated. Ensure the signature comes from the person requesting the coverage determination.
- Finally, review the completed form making sure all necessary information is filled out correctly. Save your changes, download a copy for your records, and print or share the form as needed.
Complete your coverage determination request form online today for timely processing.
Please contact the Customer Care toll free number listed on your pharmacy benefit member ID card or call Navitus Customer Care at 1-844-268-9789.