Loading
Get Fidelis Care Medication Request Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Fidelis Care Medication Request Form online
This guide provides a step-by-step approach to successfully fill out the Fidelis Care Medication Request Form online. Designed for ease of use, this form is essential for ensuring timely requests for medication through Fidelis Care.
Follow the steps to fill out the form accurately.
- Click 'Get Form' button to access the Fidelis Care Medication Request Form. This will allow you to obtain the necessary document in an editable format.
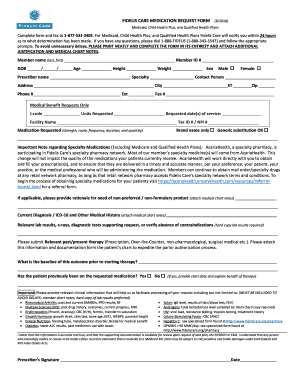
- Begin by entering the member's name, member ID, date of birth, age, height, weight, and sex. Ensure that this information is accurate and clearly printed.
- Next, provide the prescriber's name, specialty, contact person, address, city, state, zip code, phone number, extension, and fax number. Complete all required fields.
- For medical benefit requests only, fill in the J-code and units requested, along with the requested dates of service.
- Enter the facility name and associated tax ID or NPI number. Choose between 'Brand name only' or 'Generic substitution OK' as appropriate.
- Specify the medication requested, including strength, route, frequency, duration, and quantity.
- If applicable, provide rationale for needing a non-preferred or non-formulary product. Attach any relevant medical chart notes.
- Document the current diagnosis using ICD-10 codes, while also providing other pertinent medical history and attaching relevant lab results as needed.
- Note any relevant past or present therapy, including prescriptions and over-the-counter medications.
- Indicate the patient's baseline outcome prior to starting the therapy and whether the patient has been on the requested medication previously, detailing the start date and benefits observed.
- Conclude by ensuring all required clinical information is included to facilitate the processing of the request. Check that all supporting documentation is available for review.
- Finally, ensure that the prescriber signs and dates the form before submission.
Complete your Fidelis Care Medication Request Form online today to ensure timely processing of your medication requests.
Wellcare Fidelis No Premium (HMO) and Wellcare Fidelis Patriot No Premium (HMO-POS) have a network of doctors, hospitals, pharmacies, and other providers.