Loading
Get Provider Appeal Request Form - Blue Cross Blue Shield Of Rhode ...
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to use or fill out the Provider Appeal Request Form - Blue Cross Blue Shield Of Rhode Island online
Filling out the Provider Appeal Request Form is an important step in appealing a denial from Blue Cross Blue Shield of Rhode Island. This guide will provide you with clear, step-by-step instructions to help you complete the form accurately and efficiently online.
Follow the steps to effectively complete your appeal request
- Click 'Get Form' button to obtain the Provider Appeal Request Form and open it in your preferred document editor.
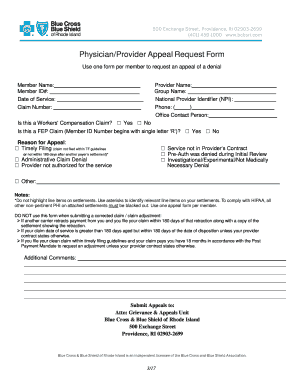
- Begin by entering the member's information in the designated fields. This includes the member name, member ID number, date of service, and claim number. Ensure that all information is accurate for a smooth processing of your appeal.
- Next, fill out the provider details. Enter the provider name, group name, National Provider Identifier (NPI), and a contact telephone number. This information helps Blue Cross Blue Shield identify the provider involved in the appeal.
- Indicate whether this appeal relates to a Workers' Compensation claim or a Federal Employee Program (FEP) claim by selecting the appropriate checkbox. This helps categorize the appeal correctly.
- In the reason for appeal section, select one or more reasons that best describe the basis for the appeal. Options include timely filing issues, service contract limitations, pre-authorization denials, investigational claims, administrative denials, or provider authorization issues. If none apply, select 'Other' and provide an explanation in the notes section.
- If needed, use the notes section for any additional comments or explanations that may support your appeal. Be concise but detailed enough to provide clarity.
- After completing all sections, review the form to ensure that all information is accurate and complete.
- Finally, save your changes, and choose whether to download, print, or share the completed form. Ensure it is submitted to the appropriate address for processing.
Start filling out your Provider Appeal Request Form online today for a timely submission.
Mail original claims to BCBSIL, P.O. Box 805107, Chicago, IL 60680-4112.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.