Loading
Get Caresource Hierarchy Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Caresource Hierarchy Form online
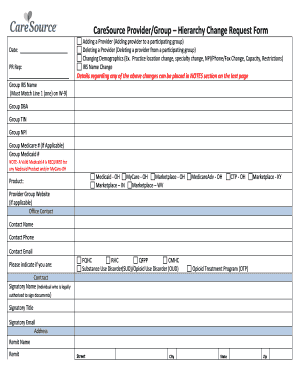
Filling out the Caresource Hierarchy Form online is an essential task for providers wishing to manage their group affiliations effectively. This guide will walk you through the process step-by-step, ensuring clarity and ease of completion.
Follow the steps to complete your Caresource Hierarchy Form with confidence.
- Press the ‘Get Form’ button to access the Caresource Hierarchy Form. Ensure that you have a stable internet connection to facilitate the download.
- Fill in the date at the top of the form, as this is essential for record-keeping.
- In the 'PR Rep' field, enter your representative’s name responsible for the submission.
- Under 'Group IRS Name', ensure that it matches line 1 of your W-9 form exactly to avoid discrepancies.
- Indicate any changes you are making, such as adding or deleting a provider, or changing demographic information, by selecting the appropriate checkboxes.
- Provide pertinent details regarding your changes in the 'NOTES' section located on the last page of the form.
- Fill in the group information including 'Group DBA', 'Group TIN', 'Group NPI', and any applicable Medicare or Medicaid numbers.
- Complete the contact section, entering the office contact’s name, phone number, and email address.
- Indicate if you are a Federally Qualified Health Center (FQHC), Rural Health Clinic (RHC), or another designation as applicable.
- For each provider being added, provide their details, including degree, specialty, contact information, and whether they provide telemedicine services.
- Ensure to specify any age or gender restrictions for the providers listed.
- At the completion of filling out the form, review your entries for accuracy.
- Finally, save your changes, and choose to download, print, or share the completed form as necessary.
Start filling out the Caresource Hierarchy Form online to ensure your group's information is accurate and up to date.
CareSource® MyCare Ohio is a Medicare-Medicaid plan that delivers extra benefits and the coordinated care needed by both patients and caregivers, giving patients more coverage and caregivers more options. QUESTIONS? GIVE US A CALL. 1-855-475-3163. (TTY: 711)
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.