Loading
Get Panfoundation Org Dmrform
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Panfoundation Org Dmrform online
This guide provides clear instructions on how to accurately complete the Panfoundation Direct Member Reimbursement (DMR) form online. Ensuring all necessary details are provided will help facilitate a smooth reimbursement process for your approved expenses.
Follow the steps to complete the DMR form effectively.
- Press the ‘Get Form’ button to access the DMR form and open it in your chosen editor.
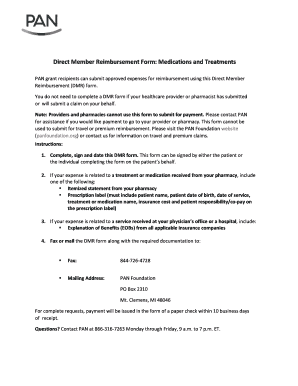
- Start by filling in the patient information section. Include the first name, last name, date of birth in MM/DD/YYYY format, PAN ID number, and group number as required.
- In the expense information section, specify the name of the medication or treatment received.
- Indicate where the medication or treatment was received by checking the appropriate box, which includes options such as physician office, pharmacy, outpatient hospital, or other.
- Record the date(s) the medication or treatment was administered, ensuring it is in the MM/DD/YYYY format.
- Enter the requested reimbursement amount clearly, as this will be the amount PAN will consider for payment.
- Select to whom the payment should be sent by checking either the patient or the caregiver/parent/guardian option, and provide the necessary name if applicable.
- Complete the address section with the street address, city, state, and ZIP code to ensure proper delivery of the payment.
- Read the declaration carefully and ensure to sign and date the form. The signature can be provided by the patient or the person completing the form on their behalf.
- Finally, attach all required documentation as outlined, including an itemized statement or prescription label for pharmacy expenses or an explanation of benefits for services received, and prepare to fax or mail the completed DMR form.
- Once all information is filled out, save your changes, and if needed, download, print, or share the form as required.
Complete your DMR form online today to ensure your reimbursement request is processed efficiently.
PAN Foundation grants provide a fast, reliable way to pay for out-of-pocket medication costs, health insurance premiums, and transportation expenses. We offer grants to help you with out-of-pocket medication copay costs, health insurance premiums, and transportation for activities that benefit your overall health.