Loading
Get Nv Prior Authorization And Referral Form 2004
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the NV Prior Authorization and Referral Form online
Filling out the NV Prior Authorization and Referral Form can seem daunting, but this guide will provide you with clear, step-by-step instructions to make the process as smooth as possible. By following these guidelines, you can ensure that all necessary information is accurately submitted online.
Follow the steps to complete the form effectively.
- Click ‘Get Form’ button to obtain the form and open it in the editor.
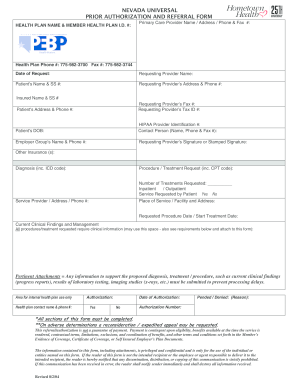
- Fill in the health plan name and member health plan identification number at the top of the form. Ensure you have the correct details to avoid processing delays.
- Enter the primary care provider's name, address, phone, and fax number in the specified fields. This information is vital for communication between healthcare providers.
- Provide the health plan's phone number and fax number, ensuring accuracy for any follow-up inquiries.
- Record the date of the request. This helps track the timeliness of the authorization process.
- Fill in the requesting provider's name along with their address and phone number. This identifies who is making the request.
- Enter the patient's name and social security number. Ensure that this information is accurate to protect patient confidentiality.
- Indicate the insured person's name and social security number, as well as the patient's address and phone number.
- Complete the sections for requesting provider's fax number and tax identification number.
- Record the patient's date of birth and the HIPAA provider identification number to maintain compliance with health information privacy standards.
- Provide the contact person's name, phone number, and fax number. This makes it easier for the health plan to reach the right person if more information is needed.
- Indicate the employer group's name and phone number to facilitate any additional communication regarding insurance coverage.
- Ensure that the requesting provider's signature or stamped signature is included to validate the request.
- List any other insurance coverage the patient may have to ensure that all benefits are considered.
- Provide the diagnosis and relevant ICD code. Accurate coding is essential for proper processing.
- Detail the procedure or treatment request along with the CPT code associated with it.
- Indicate the number of treatments requested and specify whether the request is for inpatient or outpatient services.
- Answer whether the service is requested by the patient and provide the service provider's address and phone number.
- Fill in the place of service or facility and address where the procedure will take place.
- Indicate the requested procedure date or start treatment date.
- Provide any current clinical findings and management observations. Attach supporting clinical information to prevent delays.
- In the area for internal health plan use, leave space for the health plan contact name and phone number if available.
- Indicate the authorization status, providing details if the request is pended or denied.
- Once all sections are completed, users can save changes, download, print, or share the form as needed.
Complete your forms online now to streamline your authorization process.
Get form
Experience a faster way to fill out and sign forms on the web. Access the most extensive library of templates available.
To get the NV Prior Authorization and Referral Form, start by contacting your healthcare provider or insurance company for the specific form they require. Additionally, USLegalForms offers a streamlined way to access various legal forms, including authorization forms, easily. It is beneficial to review all applicable details to avoid any delays in your healthcare services.
Get This Form Now!
Use professional pre-built templates to fill in and sign documents online faster. Get access to thousands of forms.