Loading
Get Mapd Prescription Reimbursement Request Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the MAPD prescription reimbursement request form online
The MAPD prescription reimbursement request form is an essential document for individuals seeking reimbursement for covered medications purchased at retail cost. This guide provides step-by-step instructions to help users complete the form accurately and efficiently online.
Follow the steps to successfully complete the MAPD prescription reimbursement request form online.
- Press the ‘Get Form’ button to access the MAPD prescription reimbursement request form. This will open the form in your online editor, allowing you to complete it digitally.
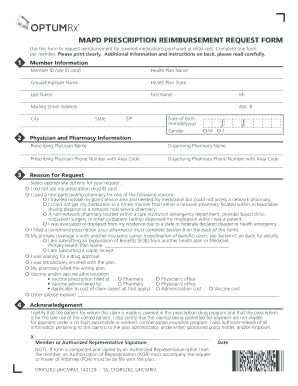
- Begin by filling out the member information section. Enter your member ID, health plan name, group/employer name, state, last name, first name, middle initial, mailing address, city, state, ZIP, date of birth in the specified format (mm/dd/yyyy), and gender.
- Provide the physician and pharmacy information. Include the prescribing physician's name, dispensing pharmacy name, and their respective phone numbers with area codes.
- In the reason for request section, check all relevant options that apply to your situation. This may include reasons related to pharmacy use, prescription types, or other circumstances.
- Read the acknowledgement carefully. By signing, you confirm that the patient is covered under the prescription drug program and that the information provided is accurate. Fill in the signature and date fields.
- Include the original pharmacy receipt for each medication. Ensure the receipts have all required information as outlined in Section A.
- Print the second page of the form on the back of the first page, if applicable.
- Send the completed form along with all required pharmacy receipts to the specified address: OptumRx Claims Department, P.O. Box 29045, Hot Springs, AR 71903. Double-check that your form is complete to avoid delays in reimbursement.
Complete the MAPD prescription reimbursement request form online to ensure a smooth and efficient reimbursement process.
Form CMS-1696 can be downloaded at .cms.gov or obtained by calling the Customer Service number on your member ID card. The claim may be submitted via mail or fax to the address or phone number on the Medicare Part D Prescription Drug Claim Form.