Loading
Get Doc-1163a Authorization For Use And Disclosure Of Protected Health Information (phi) (2)
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to use or fill out the DOC-1163A Authorization For Use And Disclosure Of Protected Health Information (PHI) (2) online
Completing the DOC-1163A Authorization For Use And Disclosure Of Protected Health Information online can be a straightforward process with the right guidance. This guide provides clear, step-by-step instructions to assist you in accurately filling out the form to ensure your protected health information (PHI) is properly managed.
Follow the steps to successfully complete the DOC-1163A form online.
- Click 'Get Form' button to download the DOC-1163A form and open it in your preferred online editor.
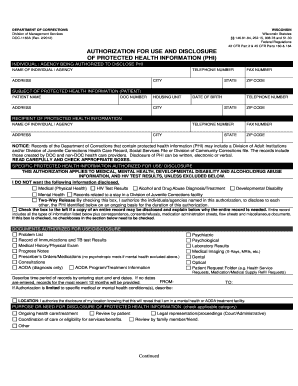
- In the first section, provide the name, telephone number, address, city, fax number, state, and zip code of the individual or agency authorized to disclose PHI.
- Next, enter the subject's details. This includes the patient name, DOC number, address, housing unit, city, date of birth, telephone number, state, and zip code.
- Complete the recipient section by filling in the name, telephone number, address, city, fax number, state, and zip code of the individual or agency receiving the PHI.
- Read the notice carefully, then indicate the specific protected health information that you want to authorize for disclosure. Select any exclusions if necessary.
- If applicable, check the two-way release box to allow sharing of PHI between identified parties, and state the reason for needing the entire record if you choose that option.
- List the documents authorized for use or disclosure by checking the relevant boxes or adding additional details in the provided field.
- Indicate the time period for which records may be disclosed by entering start and end dates. If no dates are added, the last 12 months will be provided.
- Choose the purpose or need for the disclosure of PHI by checking applicable categories such as ongoing health care or legal representation.
- At this stage, review the patient rights section to ensure you understand your rights regarding this authorization.
- Sign and date the authorization form to confirm that it accurately reflects your wishes regarding the use and disclosure of your PHI.
- Finally, save your changes, and you can opt to download, print, or digitally share the completed form as needed.
Start filling out your DOC-1163A form online today to manage your protected health information effectively.
Authorization. A covered entity must obtain the individual's written authorization for any use or disclosure of protected health information that is not for treatment, payment or health care operations or otherwise permitted or required by the Privacy Rule.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.