Loading
Get Inpatient Notice Of Discharge Form Behavioral Health Cigna-healthspring
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Inpatient Notice Of Discharge Form Behavioral Health Cigna-HealthSpring online
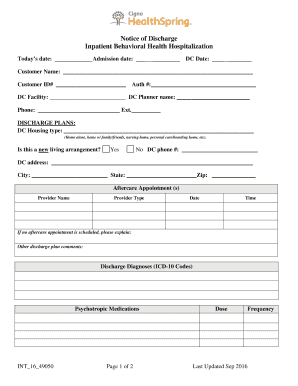
The Inpatient Notice Of Discharge Form Behavioral Health Cigna-HealthSpring is a critical document that records essential discharge information for individuals leaving inpatient care. This guide provides a clear, step-by-step approach to filling out the form online, ensuring that all necessary details are accurately captured for a smooth transition.
Follow the steps to successfully complete the form online.
- Click ‘Get Form’ button to access the form and open it for editing.
- Begin by entering today’s date in the designated field, followed by the admission date.
- Fill in the discharge date and the customer's name along with their customer ID number.
- Provide the authorization number and the discharge facility details, including the planner's name and phone number.
- Outline the discharge plans by specifying the type of housing the individual will be moving to, marking whether it is a new living arrangement.
- If applicable, fill in the discharge phone number and address fields, followed by city, state, and zip code.
- List any aftercare appointments by providing the provider's name, type, date, and time. If no appointment is scheduled, include a brief explanation.
- Add any additional comments regarding the discharge plan.
- Document the discharge diagnoses by entering the relevant ICD-10 codes and any prescribed psychotropic medications, including dosage and frequency.
- Ensure to review all entries for accuracy, then proceed to save changes, download, print, or share the completed form as required.
Complete your discharge forms online to ensure a seamless transition.
Claims — Submit claims to: Cigna Medical Claims P.O. Box 188061, Chattanooga, TN 37422-8061 Payer ID 62308 Explanation of Payment (EOP) — You'll receive an EOP for billed services with processing information for the visit.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.