Loading
Get 18004245725
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the 18004245725 online
Completing the 18004245725 form online is a straightforward process that ensures your request is submitted accurately and efficiently. This guide provides you with step-by-step instructions to help you fill out the form with ease, making sure all necessary information is included.
Follow the steps to successfully complete the form.
- Press the ‘Get Form’ button to access the form for completion.
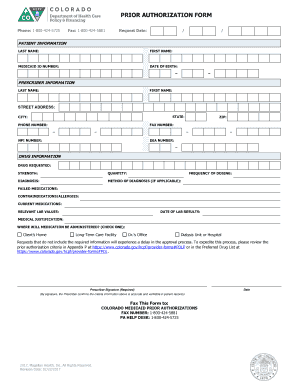
- Begin by entering the patient information in the designated fields, including last name, first name, Medicaid ID number, and date of birth.
- Provide the prescriber information, ensuring you fill out their last name, first name, street address, city, state, zip code, phone number, fax number, NPI number, and DEA number.
- In the drug information section, specify the drug requested, its strength, quantity, frequency of dosing, diagnosis, method of diagnosis (if applicable), failed medications, contraindications/allergies, current medications, relevant lab values, and the date of lab results.
- Fill out the medical justification section, detailing the reasons for the medication. This is critical for the approval process.
- Indicate where the medication will be administered by checking the relevant option, either Client’s Home, Long-Term Care Facility, Doctor’s Office, or Dialysis Unit or Hospital.
- Ensure all required information is complete to avoid delays in processing. Review the prior authorization criteria to confirm compliance.
- Obtain the prescriber’s signature in the designated area, providing confirmation that the criteria information is accurate and verifiable.
- After completing the form, you can choose to save changes, download a copy, print it for physical submission, or share it via fax to COLORADO MEDICAID PRIOR AUTHORIZATIONS at 1-800-424-5881.
Start filling out the 18004245725 form online today to ensure a smooth authorization process.
Important Phone Numbers: Health First Colorado (Colorado's Medicaid Program) Customer Service - (800) 221-3943.