Loading
Get State Form 55317 (r / 11-16)
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the State Form 55317 (R / 11-16) online
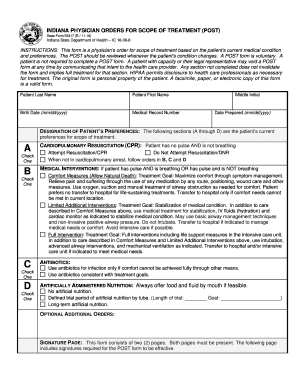
Filling out the State Form 55317 (R / 11-16), also known as the Indiana Physician Orders for Scope of Treatment (POST), can be an essential step in ensuring that a person's medical preferences are documented and respected. This guide provides clear and detailed instructions on how to complete this form online, helping users navigate its components effectively.
Follow the steps to complete the State Form 55317 online
- Click the ‘Get Form’ button to obtain the form and open it in the online editing tool.
- Begin by filling in the patient’s last name, first name, and middle initial in the designated fields. Ensure accuracy as this information is crucial for identification.
- Enter the birth date of the patient in the format mm/dd/yyyy. This is important for verifying the patient's identity and age.
- Provide the medical record number if available. This helps link the POST form to the patient’s health records.
- Indicate the date the POST form is prepared by entering it in the designated field in mm/dd/yyyy format.
- In the designation of patient’s preferences section (A through D), check the appropriate boxes to reflect the patient’s current treatment preferences.
- When filling out the cardiovascular resuscitation section, choose either 'Attempt Resuscitation/CPR' or 'Do Not Attempt Resuscitation/DNR' based on the patient’s wishes.
- For medical interventions, select one of the three options: Comfort Measures, Limited Additional Interventions, or Full Intervention, clearly indicating the desired level of treatment.
- If antibiotics are desired, designate the use of antibiotics consistent with the treatment goals, providing clear preferences if necessary.
- Specify preferences for artificially administered nutrition, choosing from 'Always offer food and fluid by mouth if feasible,' 'No artificial nutrition,' 'Defined trial period of artificial nutrition by tube,' or 'Long-term artificial nutrition.'
- If applicable, complete the signature page by writing the name of the patient or legally appointed representative, as well as the date of birth in the mm/dd/yyyy format.
- The patient or legally appointed representative must sign and date the form, ensuring it reflects the individual’s wishes.
- If the signature is that of a representative, provide their contact information, including address and telephone number.
- Complete the physician order section, ensuring it is signed by the treating physician along with their printed name, date, office telephone number, and license number.
- Review all entered information for accuracy and completeness before finalizing the form.
- Once finalized, save changes, download, print, or share the completed State Form 55317 as needed.
Get started on completing your documents online today!
The purpose of the POST form is to ensure that the patient's wishes for treatment at the end of life are followed, so a conversation must take place.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.