Get Ga Pshp Pregnancy Notification Form 2009-2026
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the GA PSHP Pregnancy Notification Form online
The GA PSHP Pregnancy Notification Form is an essential document for individuals to notify their healthcare providers and insurance plans about their pregnancy. Completing this form accurately is vital for ensuring proper care and access to necessary services during your pregnancy journey.
Follow the steps to fill out the GA PSHP Pregnancy Notification Form online
- Click ‘Get Form’ button to obtain the form and open it in your preferred editor.
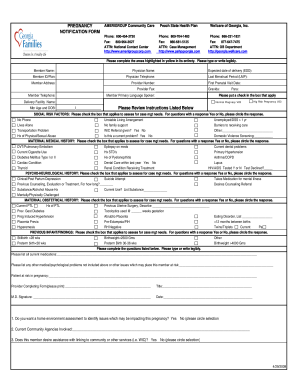
- Begin by filling in the member name, which refers to the person who is pregnant.
- Next, enter the member ID or plan number, as well as the name and telephone number of the physician.
- Complete the member address and provider number to assist with location identification.
- Indicate the expected date of delivery and the last menstrual period, along with the date of the first prenatal visit.
- Fill in the provider fax number and member telephone number for further communication.
- Specify the gravida (number of pregnancies) and para (number of births) status.
- Select the primary language spoken by the member for effective communication.
- Check the box for the delivery facility name to indicate where the birth will take place.
- Assess and mark whether this is a normal or high-risk pregnancy.
- Review and complete the social risk factors section by checking applicable boxes and circling responses for yes or no questions.
- Complete the maternal medical history section by checking the applicable conditions.
- Fill out the psycho-neurological history to indicate any mental health concerns.
- Complete maternal obstetrical history by checking appropriate past conditions related to pregnancy.
- Document any previous findings regarding infants or other relevant medical history.
- List current medications and any additional medical or psychological issues not previously mentioned.
- Provide details regarding the patient at risk in pregnancy.
- Have the provider complete the signature section along with title, date, and any required assessments or agency involvement.
- After filling out the form, review all entered information for accuracy.
- Save changes, download, print, or share the completed form as needed.
Complete the GA PSHP Pregnancy Notification Form online to ensure timely and appropriate care during your pregnancy.
A notification of pregnancy is a formal way to inform healthcare providers and insurance about your pregnancy. The GA PSHP Pregnancy Notification Form serves this purpose effectively. By submitting this form, you initiate the process to receive specialized maternal healthcare services. It ensures that you and your baby receive the support and resources you need during this important time.