Loading
Get Recurring Medicare Part B Reimbursement Request Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Recurring Medicare Part B Reimbursement Request Form online
Completing the Recurring Medicare Part B Reimbursement Request Form online is a straightforward process that ensures you receive your premium reimbursements efficiently. Follow this guide to ensure you fill out all required sections accurately and submit your request without issues.
Follow the steps to successfully complete your reimbursement request form.
- Press the ‘Get Form’ button to access the form and open it in your digital editor.
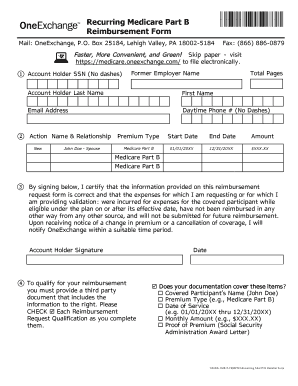
- Enter your account holder information in the corresponding fields. This includes your Social Security Number (without dashes), former employer name, total pages, last name, first name, email address, and daytime phone number.
- In the action section, indicate whether this request is 'New', 'Change', or 'End'. Enter the relationship of the account holder to the person requesting the reimbursement (e.g., self, spouse).
- Specify the premium type, which should be Medicare Part B.
- Fill in the start date for the premium, typically January 1 of the applicable year, or the date when coverage begins.
- If applicable, provide the end date for the premium, often December 31 of the applicable year, or an earlier date in case of death of the covered participant.
- Input the monthly amount for the premium matching what is shown on your supporting documentation.
- Read the certification statement carefully. By signing, you confirm that the information supplied is accurate and that you have not received reimbursement from another source.
- To qualify for reimbursement, check each required item (covered participant's name, premium type, date of service, and monthly amount) against your third-party documentation.
- After completing the form, save your changes, and you may choose to download, print, or share the form as needed.
Complete your reimbursement request form online today to streamline your Medicare Part B reimbursements.
Related links form
The Recurring Premium Reimbursement Claim Form lets you request reimbursement of your health care premiums on a recurring basis. Your premiums must be a fixed monthly amount for a set period of time.