Loading
Get Medi-cal Rendering Provider Application/disclosure Statement ...
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Medi-Cal Rendering Provider Application/Disclosure Statement online
Filling out the Medi-Cal Rendering Provider Application/Disclosure Statement online can streamline the process of submitting claims and ensure that all necessary information is accurately provided. This guide offers clear, step-by-step instructions to assist you in completing the form with ease.
Follow the steps to complete the application accurately.
- Press the ‘Get Form’ button to access the Medi-Cal Rendering Provider Application/Disclosure Statement and open it in your preferred editor.
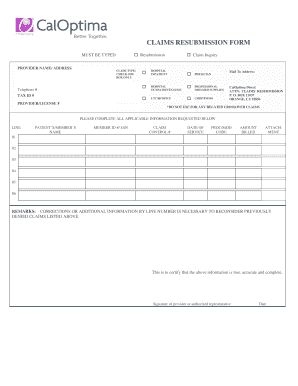
- Enter your provider name and address in the designated fields at the top of the form. Ensure that the information is typed accurately to avoid delays.
- Select your claim type by checking only one box from the options provided. This indicates the nature of your resubmission.
- Fill in your telephone number and Tax ID number in the specified sections. This information is essential for identifying your practice.
- Complete the section labeled 'Patient's/Member's Name' and provide the member ID number or Social Security Number (SSN) as applicable.
- Input the claim control number and date of service for the claims you are resubmitting. Accurate details in these fields will facilitate quicker processing.
- Enter the procedure/modifier code and the amount billed for each claim. Accuracy is crucial to prevent further issues.
- In the remarks section, provide any necessary corrections or additional information line by line that pertains to previously denied claims.
- Sign and date the form at the bottom, certifying that the information provided is true and complete.
- Once completed, save your changes and prepare to print or share the form along with any required attachments before submitting it.
Complete your Medi-Cal Rendering Provider Application/Disclosure Statement online today to ensure efficient processing of your claims.
Forms and attachments can be mailed to the address shown on the ACF or faxed to 1-866-438-9377. Each fax must include an ACF as the cover page followed by the corresponding attachment pages. Additional ACFs and attachments must be faxed separately. The ACF must be an original form obtained from Medi-Cal.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.