Loading
Get Cigna Medication Prior Authorization Form 2010
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Cigna medication prior authorization form online
Filling out the Cigna medication prior authorization form online can streamline the process of obtaining necessary medications for your patients. This guide offers clear and detailed instructions to help you navigate each section of the form effectively.
Follow the steps to complete the form accurately
- Press the ‘Get Form’ button to access the medication prior authorization form and open it in your document editor.
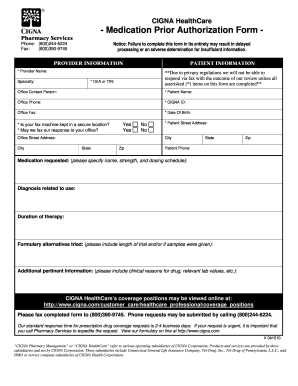
- Begin by entering your provider information in the designated fields. Include your name, specialty, DEA or TIN, and contact details. Ensure all fields marked with an asterisk (*) are filled, as incomplete forms may delay processing.
- Next, fill out the patient information section. Provide the patient's full name, Cigna ID, date of birth, and contact details. Again, be attentive to mandatory fields marked with an asterisk (*).
- In the medication requested section, specify the medication name, strength, and dosing schedule accurately. This information is crucial for the approval process.
- Describe the diagnosis related to the medication use. This assists in providing context for the necessity of the requested medication.
- Indicate the duration of therapy required. This helps Cigna evaluate the ongoing need for the medication.
- List any formulary alternatives that have been tried. Include details about the length of trials and any samples that were provided. This information supports your request.
- Provide additional pertinent information if applicable, such as clinical justification for the medication and relevant lab values.
- Review the entire form for completeness and accuracy. Once satisfied, you can save your changes, download a copy, print, or share the document as needed.
Complete the form online today to ensure timely processing of your medication requests.
Get form
Experience a faster way to fill out and sign forms on the web. Access the most extensive library of templates available.
Related links form
For assistance with the Cigna medication prior authorization form, you can contact Cigna’s customer service at their designated phone number, which you can find on their website or your insurance card. This resource can provide real-time help and information based on your needs.
Get This Form Now!
Use professional pre-built templates to fill in and sign documents online faster. Get access to thousands of forms.