Loading
Get Request For Medicare Prescription Drug Coverage Determination (ebs). Prescription Drug Coverage
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to use or fill out the REQUEST FOR MEDICARE PRESCRIPTION DRUG COVERAGE DETERMINATION (EBS) online
Filling out the Request for Medicare Prescription Drug Coverage Determination (EBS) can seem complex, but with clear guidance, you can navigate it with ease. This guide offers step-by-step instructions on how to complete the form to ensure your prescription drug coverage needs are met.
Follow the steps to effectively fill out your coverage determination request.
- Press the ‘Get Form’ button to access the form and open it in your document editor.
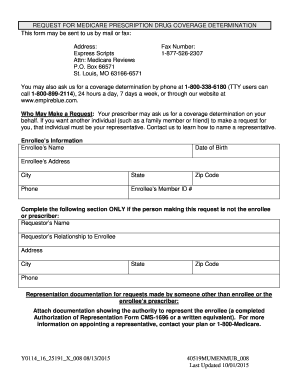
- Fill in the enrollee’s information, including the name, date of birth, address, city, state, zip code, phone number, and member ID number. Ensure all details are accurate and up to date.
- If the request is made by someone other than the enrollee or prescriber, complete the requestor's information section, which includes their name, relationship to the enrollee, address, city, state, zip code, and phone number.
- Attach any necessary representation documentation if applicable. This could be a completed Authorization of Representation Form (CMS-1696) or a written equivalent evidencing the requestor's authority to act on behalf of the enrollee.
- Indicate the name of the prescription drug you are requesting, including the strength and quantity needed per month, if known.
- Choose the type of coverage determination request that applies. There are various options, such as requesting a drug that is not on the plan’s formulary, a prior authorization, or an exception to quantity limits. Make sure to check the relevant box.
- If required, indicate any additional information that should be considered for your request. Attach any supporting documents relevant to your situation.
- If expedited decisions are necessary, check the box indicating that waiting 72 hours may harm your health. Ensure you provide the prescriber’s supporting statement if applicable.
- Complete the prescriber's information by filling in their name, address, city, state, phone number, and fax number.
- Finally, provide the prescriber's signature and date signifying their support for the request. Make sure to include any relevant diagnosis and medical information as outlined.
- Review the completed form for accuracy before submitting. You can save changes, download, print, or share the form as necessary.
Begin your online request for Medicare prescription drug coverage determination today to ensure you receive the medications you need.
How to Request a Coverage Determination. An enrollee, an enrollee's prescriber, or an enrollee's representative may request a standard or expedited coverage determination by filing a request with the plan sponsor. Standard or expedited requests for benefits may be made verbally or in writing.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.