Loading
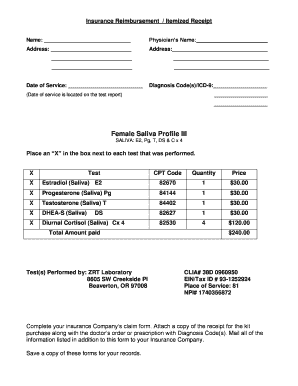
Get Insurance Reimbursement / Itemized Receipt Name: Physicians Name: Address: Address: Date Of
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the insurance reimbursement / itemized receipt online
Filling out the insurance reimbursement or itemized receipt form can be a straightforward process when you understand each section. This guide provides you with clear and precise instructions to complete the form accurately and efficiently.
Follow the steps to complete your form correctly.
- Click the ‘Get Form’ button to acquire the form and open it in your preferred editor.
- Begin filling in the 'Name' field with your full name as it appears on your insurance documentation.
- Next, enter the physician’s name in the designated field. This should be the name of the medical professional who provided the services.
- Complete the first 'Address' field with the doctor's office address. Ensure it contains the correct street name and number.
- In the second 'Address' field, include additional details, such as the suite or unit number if applicable.
- Fill in the 'Date of Service' field with the date when the medical service was performed. This information is typically found on the test report.
- In the 'Diagnosis Code(s)/ICD-9' section, list any relevant codes that relate to the services you received. Make sure to verify accuracy for submission.
- Review the tests performed and place an 'X' in the box next to each applicable test. Verify the CPT codes and quantities corresponding to the services listed.
- Ensure the 'Total Amount Paid' reflects the sum of all tests completed. Double-check your calculation for accuracy.
- Confirm that the 'Test(s) Performed by' section contains the correct laboratory name and address, and verify the CLIA and NPI numbers are listed.
- Complete your insurance company’s claim form, attaching a copy of this itemized receipt along with any supporting documents required by your insurer.
- Before submitting, save a copy of all documents for your records. Ensure all information is accurate and complete.
Start filling out your forms online today and streamline your insurance reimbursement process.
In most cases, your letter should contain: Your name. Your contact information. Insurance policy number. Details of the accident. Any injuries or damages. Any medical bills or repair estimates. Any information connected to a police report. Contact information for anyone else involved in the accident.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.