Loading
Get Reimbursement Transmittal Claim Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the reimbursement transmittal claim form online
Filling out the reimbursement transmittal claim form can be an essential step in obtaining the benefits owed to you. This guide provides step-by-step instructions to help you complete the form online effectively and accurately.
Follow the steps to complete your reimbursement transmittal claim form.
- Click ‘Get Form’ button to obtain the form and open it for editing. This action will allow you to access the necessary document to start your claim.
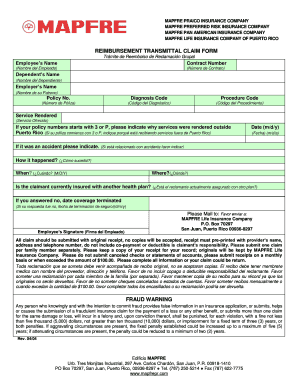
- Begin by entering the employee's name in the designated field labeled 'Employee’s Name.' Ensure that the name matches the one on the insurance policy.
- Enter your contract number in the 'Contract Number' field. This number can typically be found on your insurance documents.
- Fill in the dependent's name if applicable, in the 'Dependent’s Name' field. Include the names of anyone who is covered under the policy and involved in the claim.
- Next, input the employer's name in the corresponding section. This step helps in identifying the policyholder.
- Provide the policy number in the designated area. This number is crucial for the processing of your claim.
- Fill in the diagnosis code, which relates to the medical condition for which you are seeking reimbursement. If you are unsure, refer to your healthcare provider.
- Enter the procedure code associated with the medical service received. This can also be obtained from your healthcare provider.
- Describe the service rendered in the 'Service Rendered' section. Be specific to ensure clarity.
- If your policy number begins with 3 or P, indicate the reason for services rendered outside Puerto Rico in the specified section.
- Record the date of service in the format m/d/y. Accurate dates help validate your claim.
- If applicable, indicate if the service was due to an accident. Provide detailed information on how, when, and where the accident occurred.
- Answer whether the claimant is currently insured with another health plan. If the response is 'no,' provide the date coverage was terminated.
- Review all provided information for accuracy. Ensure every section is completed to avoid any delays in processing your claim.
- Submit all claims with the original receipt; copies will not be accepted. The receipt must display the provider’s name, address, and phone number. Keep a copy for your records.
- After completing the form, you can save your changes, download, print, or share the form as needed.
Start your reimbursement process by filling out the form online today.
Get form
Experience a faster way to fill out and sign forms on the web. Access the most extensive library of templates available.
Related links form
Colorado Sex Offender Management Board (SOMB) INTENT TO APPLY FOR THE ADULT AND JUVENILE PROVIDER
Application - Colorado State Land Board - Trustlands State Co
Temporary Access Permit Application - Colorado State Land Board - Trustlands State Co
Collateral Interest Fill-in Form - Colorado State Land Board - Trustlands State Co
Get This Form Now!
Use professional pre-built templates to fill in and sign documents online faster. Get access to thousands of forms.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.