Loading
Get Prior Authorization Request Form - Medtronicfeaturescom
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Prior Authorization Request Form - Medtronicfeaturescom online
Completing the Prior Authorization Request Form for Medtronic can seem complex, but with a clear understanding of each section, the process can be straightforward. This guide provides detailed, step-by-step instructions to help you efficiently fill out the form online.
Follow the steps to complete your form accurately.
- Click ‘Get Form’ button to access the Prior Authorization Request Form and open it in your preferred editing tool.
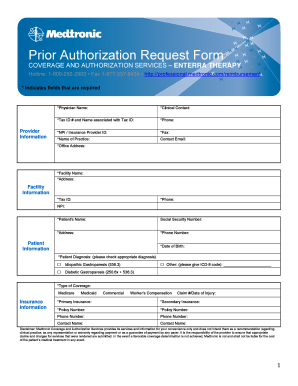
- Begin with the 'Provider Information' section. Fill in the physician's name, clinical contact, tax ID and associated name, phone number, NPI or insurance provider ID, fax, name of practice, contact email, and office address. Ensure that all required fields marked with an asterisk are completed.
- Move to the 'Patient Information' section. Input the patient’s name, social security number, address, phone number, date of birth, and diagnosis. Check the appropriate diagnosis from the options provided and ensure accurate coding.
- In the 'Insurance Information' section, specify the type of coverage (e.g., Medicare, Medicaid, Commercial). For each insurance type, provide the primary and secondary insurance details, including policy numbers and contact information.
- Fill out the 'Anticipated Service Information'. Indicate whether the procedure is for implant, revision, or replacement and specify the projected surgery date. Check all applicable procedures and indicate the physician's performance of the procedure, in-network or out-of-network settings.
- Provide answers in the 'Patient History and Nature of Disorder' section, including current symptoms, past hospitalizations related to gastroparesis, nutrition methods, frequency of nausea and vomiting, and medications tried and failed. Ensure to document all relevant medical history.
- Complete the 'Quality of Life' section by answering whether symptoms affect the patient's quality of life and providing a brief explanation if applicable.
- Once all sections are filled out, double-check for accuracy. Save your changes. You can then download, print, or share the completed form as necessary.
Start completing your forms online for a streamlined and efficient experience.
If you think more information or an additional form may be needed, please check the issuer's website before faxing or mailing your request. Please fax form to Superior HealthPlan at 1-866-399-0929.