Loading
Get Health Alliance Prior Authorization Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Health Alliance Prior Authorization Form online
Filling out the Health Alliance Prior Authorization Form is essential for obtaining approval for certain medical services. This guide provides clear and detailed instructions to support users in completing the form accurately and efficiently online.
Follow the steps to fill out the form effectively.
- Click 'Get Form' button to access the Health Alliance Prior Authorization Form and open it in your preferred online editor.
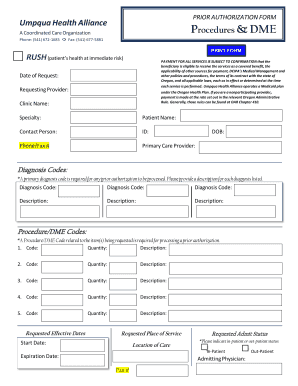
- Begin by filling out the 'Date of Request' field with the current date. This helps to track the timing of the authorization request.
- Enter the 'Requesting Provider' information. This should include the name of the provider who is requesting the authorization.
- Complete the 'Clinic Name' and 'Specialty' fields with the relevant details pertaining to the healthcare provider or organization.
- Fill in the 'Patient Name' section with the full name of the individual requiring services.
- Add the 'Contact Person' details, which could be a family member or healthcare staff who can be contacted for further information.
- Input the 'Patient ID' and 'Phone/Fax #' fields to ensure proper communication with the healthcare facility.
- Provide the name of the 'Primary Care Provider' and their details, as necessary.
- Fill in the 'DOB' (date of birth) of the patient to verify their identity and age.
- List the 'Diagnosis Codes'. You must include a primary diagnosis code as it is necessary for processing the request. Provide a description for each code listed.
- Enter the 'Procedure/DME Codes'. You must specify at least one code related to the items being requested. Include the quantity and a description for each item.
- Indicate the 'Requested Admit Status' by selecting either 'In-Patient' or 'Out-Patient'. This is crucial for determining the nature of the request.
- Fill in the 'Start Date' and 'Expiration Date' for the services requested.
- Complete the 'Admitting Physician' section with their name and fax number if applicable.
- Once all fields are completed, review your entries for accuracy. Save your changes, download a copy of the filled form, or print it for submission.
Get started now by completing the Health Alliance Prior Authorization Form online for your medical services.
COB exists when an enrollee is also covered by another plan and determines which plan pays first. The COB provision applies when you or your covered Dependent have health care coverage under more than one plan.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.