Loading
Get Aca Health Claim Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the ACA Health Claim Form online
The ACA Health Claim Form is an essential document for users to submit their health insurance claims effectively. This guide provides a comprehensive overview of how to fill out the form online, ensuring that you can navigate each section with confidence and ease.
Follow the steps to complete your ACA Health Claim Form online.
- Click ‘Get Form’ button to obtain the ACA Health Claim Form and open it in your preferred editor.
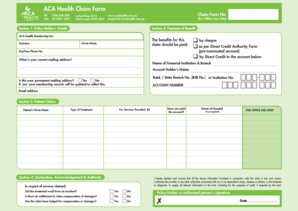
- In Section 1, enter the policy holder's details including their ACA Health Membership Number, surname, given name, daytime phone number, and email address. Make sure to verify the accuracy of the details provided.
- Still in Section 1, provide your current mailing address. Indicate whether this is your permanent mailing address by selecting 'Yes' or 'No.' If 'Yes', your membership records will be updated.
- In Section 2, choose how you would like the benefits from this claim to be paid. You can select from options such as by cheque, through direct credit to your pre-nominated account, or directly to another specified account. Fill out the required banking details including the name of the financial institution, account holder’s name, BSB number, and account number.
- Proceed to Section 3 to provide patient claims details, including the patient's given name, the name of the hospital (if applicable), and the type of treatment received. Ensure that all information accurately reflects the services provided.
- In Section 4, make the necessary declarations. Confirm if you have paid the account for the services provided or whether the treatment resulted from an accident. You will also need to indicate if there is any entitlement to claim compensation.
- Finally, check the declaration statement to ensure that all information is true and accurate. Sign with the policy holder or authorized person's signature and date the form. Review the entire form for completeness before submission.
- Once all sections are filled out and verified, save your changes, then download, print, or share the form as needed. Make sure to attach any original accounts and receipts related to the services received before mailing your claim.
Start filling out your ACA Health Claim Form online today for a smoother claims process.
used for Medicare only. It is used when a physician pays an outside entity to perform a service. If the physician has an agreement to pay for the service himself and he wants to be reimbursed for the service, he will mark "yes" and enter the amount he paid for it.