Loading
Get Prescription Claim Form - Bscmebforgb
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Prescription Claim Form - Bscmebforgb online
Completing the Prescription Claim Form - Bscmebforgb online is essential for members of the Suffolk County Municipal Employees Benefit Fund to claim prescription drug co-payment reimbursements. This guide is designed to provide clear and supportive instructions to help you navigate the form easily.
Follow the steps to accurately complete your claim form
- Click ‘Get Form’ button to obtain the form and open it in the editor.
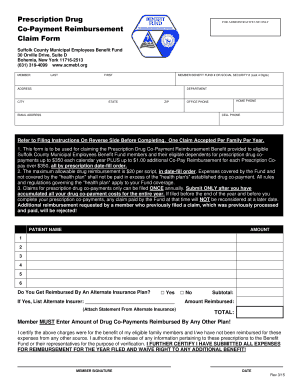
- Fill in the member's personal information, including last name, first name, member benefit fund number or last four digits of the social security number, address, city, state, zip code, home phone, office phone, email address, and cell phone.
- Complete the patient name field by listing each eligible family member receiving medication.
- Indicate the amount for each prescription co-payment claimed, up to the maximum allowable reimbursement.
- If applicable, specify if you are reimbursed by an alternate insurance plan by selecting the appropriate box and listing the name of the alternate insurer.
- Ensure all required proof of payment is attached to the claim and calculate the subtotal, amount reimbursed, and the total reimbursement request.
- Sign and date the form at the bottom, certifying that the charges were for eligible family members and that you have not received reimbursement from any other source.
- Review your completed form thoroughly, ensuring all information is accurate before submitting your claim.
- Once satisfied with your completion, save changes, download, print, or share the form as required.
Start your online document submission today to ensure your prescription claims are processed promptly.
How do I send Express Scripts a new prescription? Your doctor's office can send your prescription to us electronically from their office or by fax. Go to Forms & Cards under Benefits in the top menu of the home page and select the appropriate form. your prescription to the address listed.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.