Loading
Get Health Care Claim Form - Welcome To Encon
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to use or fill out the Health Care Claim Form - Welcome To ENCON online
The Health Care Claim Form - Welcome To ENCON is essential for submitting health care claims. This guide provides a step-by-step approach to help users effectively complete the form online, ensuring accuracy and completeness.
Follow the steps to smoothly complete your claim form.
- Click ‘Get Form’ button to obtain the form and open it in the editor.
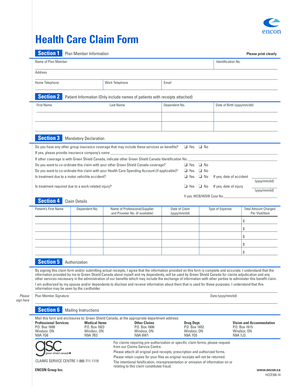
- In Section 1, enter the plan member information. This includes the name of the plan member, identification number, address, and home telephone number. Ensure that all details are printed clearly for easy readability.
- Proceed to Section 2 to provide work telephone information and patient information. List only the patients for whom you have attached receipts. Input their first and last names, dependent number, and date of birth in the format yyyy/mm/dd.
- In Section 3, complete the mandatory declaration. Indicate whether there is any other group insurance coverage that may include these services. If yes, provide the insurance company’s name and any relevant identification numbers. Also, indicate if you wish to coordinate the claim with other coverage or account.
- Section 4 is for claim details. Enter the patient’s first name, dependent number, name of the health professional or supplier, date of the claim, type of expense, and the total amount charged per visit/item. Ensure all amounts are accurately listed.
- Move on to Section 5 to authorize the claim. By signing, you confirm that the information provided is complete and accurate. Include your signature and date the form in the designated sections.
- Lastly, Section 6 includes mailing instructions. Ensure you send the completed form and any required enclosures to the correct mailing address for Green Shield Canada. Retain copies of all documents for your records, as original receipts will not be returned.
- After filling out all the required fields, save your changes, download a copy for your records, print the form if needed, or share it as required.
Start filling out your Health Care Claim Form online today to ensure timely processing of your claims.
The HCFA 1500 claim form, also known as CMS-1500, enables medical physicians to submit health insurance claims for reimbursement from various government insurance plans including Medicare, Medicaid and Tricare.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.