Loading
Get Precertification Request Form - Azblue
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the PRECERTIFICATION REQUEST FORM - AZBlue online
This guide provides comprehensive instructions on completing the PRECERTIFICATION REQUEST FORM - AZBlue online. By following these steps, users can ensure that they accurately provide all necessary information for their request.
Follow the steps to complete the form effectively.
- Click ‘Get Form’ button to access the PRECERTIFICATION REQUEST FORM - AZBlue and open it for editing.
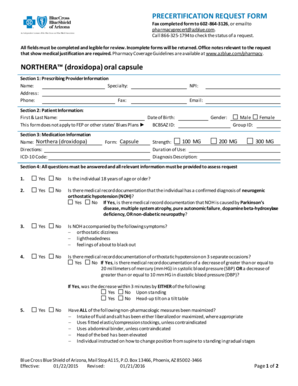
- In Section 1, fill in the prescribing provider's information, including their name, specialty, address, phone number, fax number, NPI, and email address.
- Move to Section 2 where you will provide patient information. This includes the patient's first and last name, date of birth, and BCBSAZ ID. Ensure clarity as this form does not apply to FEP or other Blues Plans.
- In Section 3, input medication information, specifying the medication name (), dosage directions, ICD-10 code, form (capsule), strength (100 MG, 200 MG, or 300 MG), duration of use, and diagnosis description.
- Address all questions in Section 4, ensuring that all relevant information that supports the request is included. This section requires detailed medical history and conditions regarding neurogenic orthostatic hypotension. Answer all questions accurately, as this is critical for the assessment.
- In Section 5, the prescribing provider must sign and date the form, affirming that all provided information is true and accurate.
- Lastly, choose the turn-around time for review in Section 6 by checking the appropriate option: standard, urgent, or exigent.
- Once all fields are completed and reviewed for clarity and accuracy, save the form changes, and prepare to either download, print, or share the completed document.
Complete your PRECERTIFICATION REQUEST FORM - AZBlue online today to ensure a smooth and efficient submission process.
Submit claims electronically to BCBSAZ (EDI Payer ID: 53589).