Loading
Get Instructions All Sections Need To Be Completed To Be A Valid Authorization
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Instructions All Sections Need To Be Completed To Be A Valid Authorization online
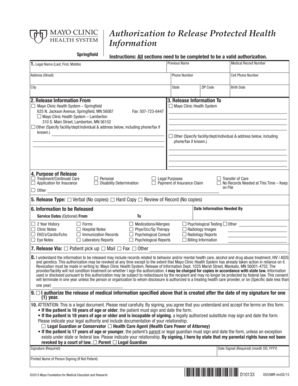
Completing the authorization to release protected health information is a vital process to ensure that your medical records are shared appropriately. This guide will help you navigate each section of the form with clear instructions, ensuring it is filled out correctly and completely.
Follow the steps to accurately complete your authorization form.
- Click ‘Get Form’ button to obtain the form and open it in the editor.
- Complete the legal name section by entering the patient's full legal name, including last, first, and middle names. Include any previous names in the designated field.
- Fill in the patient’s address, including street, city, state, and ZIP code, along with their phone number and cell phone number.
- In the release information section, specify the facility or individual from whom the records are being requested. Check off the appropriate Mayo Clinic Health System facilities, or choose 'Other' to include different entities, providing their address and contact information.
- Define to whom the information will be released by entering their name and address. If it’s another Mayo Clinic facility, check the appropriate box.
- Clarify the purpose of the release by selecting one of the options provided, or choose 'Other' and detail the reason.
- Indicate the release type by selecting whether the information will be provided verbally, as a hard copy, or through a review of the records.
- Specify the information to be released by checking the relevant types of records needed, and include the date by which the information is required.
- Choose how the information will be released, whether by mail, fax, patient pickup, or other means.
- Acknowledge understanding of the information released may pertain to sensitive health records by checking the appropriate box.
- Sign and date the form, ensuring to include your printed name if you are not the patient. If a representative is signing, documentation of their legal authority should be attached.
- Review the completed form for accuracy and clarity, then save your changes, download a copy, print it, or share it as needed.
Complete your authorization form online to ensure your medical records are shared with the right parties.
Related links form
The complete name of the person or entity to receive the protected health information (PHI) A specific description of the information to be used or disclosed, including the dates of service. The purpose of the requested use and disclosure.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.