Loading
Get Change In Provider Information - Carefirst
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Change In Provider Information - CareFirst online
Filling out the Change In Provider Information form for CareFirst is an essential process for ensuring that provider details are accurate and up-to-date. This guide will help you navigate through the online form efficiently and successfully.
Follow the steps to complete the form correctly.
- Click the ‘Get Form’ button to obtain the Change In Provider Information form and open it in your preferred editor.
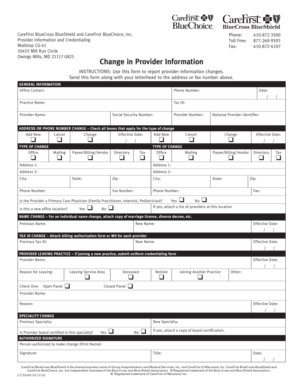
- Provide general information by filling in the office contact name, phone number, practice name, tax ID, date, provider name, social security number, and provider number.
- Indicate any address or phone number changes by checking the appropriate boxes and supplying the effective date. Specify whether you are adding new information, canceling existing information, or changing current details.
- For type of change, select from options such as office changes, mailing changes, payee/billing/vendor changes, directory changes, and tax changes, and provide the relevant address or phone number details.
- If you are reporting a name change, enter the previous and new names, along with the effective date, and attach supporting documentation like a marriage license or divorce decree.
- If you are changing your tax ID, provide the previous tax ID, new tax ID, and effective date. Attach the necessary billing authorization form or W9 for each provider.
- If a provider is leaving the practice, include their name, effective date, and the reason for leaving, selecting from the provided reasons.
- If there is a specialty change, note the previous specialty, new specialty, and indicate if the provider is board certified in this specialty. If so, attach a copy of board certification.
- Lastly, ensure the authorized signature is printed, signed, and dated by the person authorized to make the change.
- After completing the form, make sure to save your changes, download, print, or share the form as needed.
Complete your Change In Provider Information form online now to ensure accurate updates!
If you have comments or questions, we want to help you. For technical support, call the CareFirst Help Desk at (877) 526 – 8390. Below is a list that may assist you with your CareFirst provider-related questions. Contact our Credentialing Department to become a participating provider.