Loading
Get All Prior Authorization Requests Must Either Be Faxed On This Template Or Be Submitted Through The
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the All Prior Authorization Requests Must Either Be Faxed On This Template Or Be Submitted Through The online
This guide provides comprehensive instructions on completing the All Prior Authorization Requests form for physical and occupational therapy requests. Ensuring that each section is filled out correctly is essential for timely approval.
Follow the steps to effectively complete the authorization request form.
- Press the ‘Get Form’ button to access the authorization request form and open it in your preferred document editor.
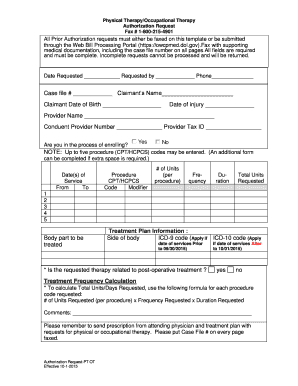
- Fill in the 'Date Requested' field with the current date, followed by the 'Requested by' section with your name and phone number.
- Enter the 'Case file #' provided for your request, then fill in the 'Claimant’s Name' and 'Claimant Date of Birth.'
- Provide the 'Date of Injury' relevant to the authorization request.
- Complete the 'Provider Name,' 'Conduent Provider Number,' and 'Provider Tax ID.'
- Indicate whether you are in the process of enrolling by selecting 'Yes' or 'No' in the appropriate field.
- For the procedure codes, enter up to five 'CPT/HCPCS' codes and respective details across all sections, including 'Date(s) of Service,' '# of Units,' 'Frequency,' and 'Duration.' Each procedure should be clearly categorized.
- Specify the 'Body part to be treated' within the appropriate section.
- For 'Treatment Plan Information,' include details for the 'Side of body' and enter the appropriate 'ICD-9 code' or 'ICD-10 code' based on the date of service.
- Indicate if the requested therapy is related to post-operative treatment by selecting 'Yes' or 'No.'
- To calculate 'Total Units/Days Requested,' use the formula: # of Units Requested (per procedure) x Frequency Requested x Duration Requested for each procedure code.
- Complete any additional comments, ensuring any critical information is included.
- Finally, remember to attach a prescription from the attending physician along with the treatment plan, ensuring the 'Case File #' is on every page before faxing the form.
Complete your authorization request now to expedite the approval process.
L.A. Care is the health plan for Medi-Cal members in Los Angeles County .
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.