Loading
Get Wc164 - Physician's Report Of Workers' Compensation Injury - Colorado
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the WC164 - Physician's Report Of Workers' Compensation Injury - Colorado online
The WC164 form is essential for accurately reporting workers' compensation injuries in Colorado. This guide offers step-by-step instructions to help users complete the form efficiently and effectively, ensuring a smooth online filing process.
Follow the steps to fill out the WC164 form correctly and efficiently.
- Click ‘Get Form’ button to obtain the WC164 form and open it in your preferred editor.
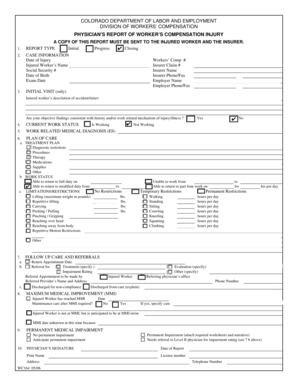
- Begin with the report type section. Indicate whether this is an 'Initial,' 'Progress,' or 'Closing' report by checking the appropriate box.
- Next, complete the case information fields. Provide the date of injury, injured worker's name, social security number, date of birth, exam date, workers' compensation number, insurer claim number, insurer name, and their phone/fax numbers, as well as the employer's details.
- In the initial visit section, include the injured worker's description of the accident/injury and confirm whether the physician's objective findings are consistent with the reported history.
- Update the current work status of the injured worker, noting if they are working or not.
- Document the work-related medical diagnosis of the injured worker in the designated field.
- Outline the plan of care by detailing the treatment plan, which may include diagnostic tools/tests, procedures, therapy, medications, supplies, and any other treatments.
- Indicate the work status—confirm if the injured worker can return to full or modified duty, specifying relevant dates. Include any limitations or restrictions on physical activities such as lifting or repetitive motion.
- Record the follow-up care and referrals by providing a return appointment date and any referrals made, along with the necessary contact information for the referred provider.
- Assess maximum medical improvement (MMI) and indicate if maintenance care is required. Provide any necessary follow-up information.
- Specify whether there is permanent medical impairment and attach any required worksheets and narratives if applicable.
- Finally, ensure the physician responsible for the report signs, dates, and includes their printed name, license number, address, and telephone number.
Complete your WC164 form online now to ensure timely and accurate workers' compensation reporting.
Form WC 1 Employer's First Report of Injury. All injuries or occupational diseases that result in lost time from work in excess of three shifts or calendar days or from permanent physical impairment must be reported to EMPLOYERS® on this form within 10 days after notice or knowledge of the injury or disease.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.